|
|
 |
| ............................................................. |
|
October 2017 -
Volume 15, Issue 8
|
 |
|
View
this issue in pdf formnat - the issue
has been split into two files for downloading
due to its large size: FULLpdf
(12 MB)
Part
1 &
Part
2
|
|
| ........................................................ |
| From
the Editor |

|
Editorial
A. Abyad (Chief Editor) |
........................................................
|
|
Original Contribution/Clinical Investigation
Immunity
level to diphtheria in beta thalassemia patients
DOI: 10.5742/MEWFM.2017.93048
[pdf
version]
Abdolreza Sotoodeh Jahromi, Karamatollah Rahmanian,
Abdolali Sapidkar, Hassan Zabetian, Alireza
Yusefi, Farshid Kafilzadeh, Mohammad Kargar,
Marzieh Jamalidoust,
Abdolhossein Madani
Genetic
Variants of Toll Like Receptor-4 in Patients
with Premature Coronary Artery Disease, South
of Iran
DOI: 10.5742/MEWFM.2017.93049
[pdf
version]
Saeideh Erfanian, Mohammad Shojaei, Fatemeh
Mehdizadeh, Abdolreza Sotoodeh Jahromi, Abdolhossein
Madani, Mohammad Hojjat-Farsangi
Comparison
of postoperative bleeding in patients undergoing
coronary artery bypass surgery in two groups
taking aspirin and aspirin plus CLS clopidogrel
DOI: 10.5742/MEWFM.2017.93050
[pdf
version]
Ali Pooria, Hassan Teimouri, Mostafa Cheraghi,
Babak Baharvand Ahmadi, Mehrdad Namdari, Reza
Alipoor
Comparison
of lower uterine segment thickness among nulliparous
pregnant women without uterine scar and pregnant
women with previous cesarean section: ultrasound
study
DOI: 10.5742/MEWFM.2017.93051
[pdf version]
Taravat Fakheri, Irandokht Alimohammadi, Nazanin
Farshchian, Maryam Hematti,
Anisodowleh Nankali, Farahnaz Keshavarzi, Soheil
Saeidiborojeni
Effect
of Environmental and Behavioral Interventions
on Physiological and Behavioral Responses of
Premature Neonates Candidates Admitted for Intravenous
Catheter Insertion in Neonatal Intensive Care
Units
DOI: 10.5742/MEWFM.2017.93052
[pdf
version]
Shohreh Taheri, Maryam Marofi, Anahita Masoumpoor,
Malihe Nasiri
Effect
of 8 weeks Rhythmic aerobic exercise on serum
Resistin and body mass index of overweight and
obese women
DOI: 10.5742/MEWFM.2017.93053
[pdf
version]
Khadijeh Molaei, Ahmad Shahdadi, Reza Delavar
Study
of changes in leptin and body mass composition
with overweight and obesity following 8 weeks
of Aerobic exercise
DOI: 10.5742/MEWFM.2017.93054
[pdf
version]
Khadijeh Molaei, Abbas Salehikia
A reassessment
of factor structure of the Short Form Health
Survey (SF-36): A comparative approach
DOI: 10.5742/MEWFM.2017.93088
[pdf version]
Vida Alizad, Manouchehr Azkhosh, Ali Asgari,
Karyn Gonano
Population and Community Studies
Evaluation
of seizures in pregnant women in Kerman - Iran
DOI: 10.5742/MEWFM.2017.93056
[pdf
version]
Hossein Ali Ebrahimi, Elahe Arabpour, Kaveh
Shafeie, Narges Khanjani
Studying
the relation of quality work life with socio-economic
status and general health among the employees
of Tehran University of Medical Sciences (TUMS)
in 2015
DOI: 10.5742/MEWFM.2017.93057
[pdf version]
Hossein Dargahi, Samereh Yaghobian, Seyedeh
Hoda Mousavi, Majid Shekari Darbandi, Soheil
Mokhtari, Mohsen Mohammadi, Seyede Fateme Hosseini
Factors
that encourage early marriage and motherhood
from the perspective of Iranian adolescent mothers:
a qualitative study
DOI: 10.5742/MEWFM.2017.93058
[pdf
version]
Maasoumeh Mangeli, Masoud Rayyani, Mohammad
Ali Cheraghi, Batool Tirgari
The
Effectiveness of Cognitive-Existential Group
Therapy on Reducing Existential Anxiety in the
Elderly
DOI: 10.5742/MEWFM.2017.93059
[pdf
version]
Somayeh Barekati, Bahman Bahmani, Maede Naghiyaaee,
Mahgam Afrasiabi, Roya Marsa
Post-mortem
Distribution of Morphine in Cadavers Body Fluids
DOI: 10.5742/MEWFM.2017.93060
[pdf
version]
Ramin Elmi, Mitra Akbari, Jaber Gharehdaghi,
Ardeshir Sheikhazadi, Saeed Padidar, Shirin
Elmi
Application
of Social Networks to Support Students' Language
Learning Skills in Blended Approach
DOI: 10.5742/MEWFM.2017.93061
[pdf
version]
Fatemeh Jafarkhani, Zahra Jamebozorg, Maryam
Brahman
The
Relationship between Chronic Pain and Obesity:
The Mediating Role of Anxiety
DOI: 10.5742/MEWFM.2017.93062
[pdf
version]
Leila Shateri, Hamid Shamsipour, Zahra Hoshyari,
Elnaz Mousavi, Leila Saleck, Faezeh Ojagh
Implementation
status of moral codes among nurses
DOI: 10.5742/MEWFM.2017.93063
[pdf
version]
Maryam Ban, Hojat Zareh Houshyari Khah, Marzieh
Ghassemi, Sajedeh Mousaviasl, Mohammad Khavasi,
Narjes Asadi, Mohammad Amin Harizavi, Saeedeh
Elhami
The comparison
of quality of life, self-efficacy and resiliency
in infertile and fertile women
DOI: 10.5742/MEWFM.2017.93064
[pdf version]
Mahya Shamsi Sani, Mohammadreza Tamannaeifar
Brain MRI Findings in Children (2-4 years old)
with Autism
DOI: 10.5742/MEWFM.2017.93055
[pdf
version]
Mohammad Hasan Mohammadi, Farah Ashraf Zadeh,
Javad Akhondian, Maryam Hojjati,
Mehdi Momennezhad
Reviews
TECTA gene function and hearing: a review
DOI: 10.5742/MEWFM.2017.93065
[pdf version]
Morteza Hashemzadeh-Chaleshtori, Fahimeh Moradi,
Raziyeh Karami-Eshkaftaki,
Samira Asgharzade
Mandibular
canal & its incisive branch: A CBCT study
DOI: 10.5742/MEWFM.2017.93066
[pdf
version]
Sina Haghanifar, Ehsan Moudi, Ali Bijani, Somayyehsadat
Lavasani, Ahmadreza Lameh
The
role of Astronomy education in daily life
DOI: 10.5742/MEWFM.2017.93067
[pdf
version]
Ashrafoalsadat Shekarbaghani
Human brain
functional connectivity in resting-state fMRI
data across the range of weeks
DOI: 10.5742/MEWFM.2017.93068
[pdf version]
Nasrin Borumandnia, Hamid Alavi Majd, Farid
Zayeri, Ahmad Reza Baghestani,
Mohammad Tabatabaee, Fariborz Faegh
International Health Affairs
A
brief review of the components of national strategies
for suicide prevention suggested by the World
Health Organization
DOI: 10.5742/MEWFM.2017.93069
[pdf
version]
Mohsen Rezaeian
Education and Training
Evaluating
the Process of Recruiting Faculty Members in
Universities and Higher Education and Research
Institutes Affiliated to Ministry of Health
and Medical Education in Iran
DOI: 10.5742/MEWFM.2017.93070
[pdf
version]
Abdolreza Gilavand
Comparison
of spiritual well-being and social health among
the students attending group and individual
religious rites
DOI: 10.5742/MEWFM.2017.93071
[pdf
version]
Masoud Nikfarjam, Saeid Heidari-Soureshjani,
Abolfazl Khoshdel, Parisa Asmand, Forouzan Ganji
A
Comparative Study of Motivation for Major Choices
between Nursing and Midwifery Students at Bushehr
University of Medical Sciences
DOI: 10.5742/MEWFM.2017.93072
[pdf
version]
Farzaneh Norouzi, Shahnaz Pouladi, Razieh Bagherzadeh
Clinical Research and Methods
Barriers
to the management of ventilator-associated pneumonia:
A qualitative study of critical care nurses'
experiences
DOI: 10.5742/MEWFM.2017.93073
[pdf version]
Fereshteh Rashnou, Tahereh Toulabi, Shirin Hasanvand,
Mohammad Javad Tarrahi
Clinical
Risk Index for Neonates II score for the prediction
of mortality risk in premature neonates with
very low birth weight
DOI: 10.5742/MEWFM.2017.93074
[pdf
version]
Azadeh Jafrasteh, Parastoo Baharvand, Fatemeh
Karami
Effect
of pre-colporrhaphic physiotherapy on the outcomes
of women with pelvic organ prolapse
DOI: 10.5742/MEWFM.2017.93075
[pdf
version]
Mahnaz Yavangi, Tahereh Mahmoodvand, Saeid Heidari-Soureshjani
The
effect of Hypertonic Dextrose injection on the
control of pains associated with knee osteoarthritis
DOI: 10.5742/MEWFM.2017.93076
[pdf
version]
Mahshid Ghasemi, Faranak Behnaz, Mohammadreza
Minator Sajjadi, Reza Zandi,
Masoud Hashemi
Evaluation
of Psycho-Social Factors Influential on Emotional
Divorce among Attendants to Social Emergency
Services
DOI: 10.5742/MEWFM.2017.93077
[pdf
version]
Farangis Soltanian
Models and Systems of Health Care
Organizational
Justice and Trust Perceptions: A Comparison
of Nurses in public and private hospitals
DOI: 10.5742/MEWFM.2017.93078
[pdf
version]
Mahboobeh Rajabi, Zahra Esmaeli Abdar, Leila
Agoush
Case series and Case reports
Evaluation
of Blood Levels of Leptin Hormone Before and
After the Treatment with Metformin
DOI: 10.5742/MEWFM.2017.93079
[pdf
version]
Elham Jafarpour
Etiology,
Epidemiologic Characteristics and Clinical Pattern
of Children with Febrile Convulsion Admitted
to Hospitals of Germi and Parsabad towns in
2016
DOI: 10.5742/MEWFM.2017.93080
[pdf
version]
Mehri SeyedJavadi, Roghayeh Naseri, Shohreh
Moshfeghi, Irandokht Allahyari, Vahid Izadi,
Raheleh Mohammadi,
Faculty development
The
comparison of the effect of two different teaching
methods of role-playing and video feedback on
learning Cardiopulmonary Resuscitation (CPR)
DOI: 10.5742/MEWFM.2017.93081
[pdf
version]
Yasamin Hacham Bachari, Leila Fahkarzadeh, Abdol
Ali Shariati
Office based family medicine
Effectiveness
of Group Counseling With Acceptance and Commitment
Therapy Approach on Couples' Marital Adjustment
DOI: 10.5742/MEWFM.2017.93082
[pdf
version]
Arash Ziapour, Fatmeh Mahmoodi, Fatemeh Dehghan,
Seyed Mehdi Hoseini Mehdi Abadi,
Edris Azami, Mohsen Rezaei
|
|
Chief
Editor -
Abdulrazak
Abyad
MD, MPH, MBA, AGSF, AFCHSE
.........................................................
Editorial
Office -
Abyad Medical Center & Middle East Longevity
Institute
Azmi Street, Abdo Center,
PO BOX 618
Tripoli, Lebanon
Phone: (961) 6-443684
Fax: (961) 6-443685
Email:
aabyad@cyberia.net.lb
.........................................................
Publisher
-
Lesley
Pocock
medi+WORLD International
11 Colston Avenue,
Sherbrooke 3789
AUSTRALIA
Phone: +61 (3) 9005 9847
Fax: +61 (3) 9012 5857
Email:
lesleypocock@mediworld.com.au
.........................................................
Editorial
Enquiries -
abyad@cyberia.net.lb
.........................................................
Advertising
Enquiries -
lesleypocock@mediworld.com.au
.........................................................
While all
efforts have been made to ensure the accuracy
of the information in this journal, opinions
expressed are those of the authors and do not
necessarily reflect the views of The Publishers,
Editor or the Editorial Board. The publishers,
Editor and Editorial Board cannot be held responsible
for errors or any consequences arising from
the use of information contained in this journal;
or the views and opinions expressed. Publication
of any advertisements does not constitute any
endorsement by the Publishers and Editors of
the product advertised.
The contents
of this journal are copyright. Apart from any
fair dealing for purposes of private study,
research, criticism or review, as permitted
under the Australian Copyright Act, no part
of this program may be reproduced without the
permission of the publisher.
|
|
|
| October 2017 -
Volume 15, Issue 8 |
|
|
A reassessment of factor
structure of the Short Form Health Survey (SF-36):
A comparative approach
Vida Alizad (1)
Manouchehr Azkhosh (2)
Ali Asgari (3)
Karyn Gonano (4)
(1) Iranian
Research Center on Ageing, University of Social
Welfare and Rehabilitation Sciences, Koodakyar
St., Daneshjou Blvd, Evin, Tehran, Iran.
(2) Counseling Department, The University of
Social Welfare and Rehabilitation Sciences,
Koodakyar St., Daneshjou Blvd, Evin, Tehran,
Iran.
(3) Department of Educational Psychology, the
University of Kharazmi, Tehran, Iran.
(4) Academic Language and Learning Services,
Queensland University of Technology, Floor 3,
X Block, Gardens Point Campus, Brisbane QLD
4000, Australia
Correspondence:
Manouchehr
Azkhosh Counseling Department,
The University of Social Welfare and Rehabilitation
Sciences,
Koodakyar St., Daneshjou Blvd, Evin,
Tehran, Iran.
Email: azkhosh34@yahoo.com
|
Abstract
Background: The factor
structure of the Short Form Health Survey
(SF-36) and its application to older people
in Eastern countries has been the focus
of limited research. Four theoretical
and experimental factor structures of
the SF-36 were tested and compared here
to establish a best-fitting model for
Iranian older people.
Methods:
A sample of 391 participants (60 -89 years)
years completed the Farsi SF-36. A confirmatory
factor analysis assessed the fit and viability
of the measurement model. Three theoretical
and experimental factor structures of
the SF-36 were tested using an exploratory
principal component analysis to explore
the factor solution of the Farsi SF-36.
Results: An
exploratory factor analysis identified
the two factor solutions (mental and physical)
to be the same as the original US model,
but the fit indices of the confirmatory
factor analysis identified the two and
three factor model (mental, physical and
well-being) to be the same, making the
latter more extensive for use with older
people.
Conclusion:
This study provides strong evidence that
the Farsi SF-36 has the potential to measure
well-being status of older people. Such
an application is valid if the Vitality
items are modified and new items are developed
for the Well-being scale.
Key words:
Health–related Quality of life, SF-36
Health Survey, older people
|
Measuring the health-related quality of life
(HRQoL) of older people has a prominent position
in gerontology as an indicator for monitoring
the health status of older people. Such monitoring
forms the basis for clinical decision-making
and gerontological research outcome measures.
Of the several instruments for measuring HRQoL,
the SF-36 Health Survey is the most widely used
in health research (1, 2) and is known for its
high standard of reliability and validity (3,
4). The SF-36 accentuates both the practical
and popular nature of the questionnaire in both
clinical settings and research. It has been
translated into more than 20 languages (5).
The SF-36 enables policy makers to involve older
people in the decision making process about
their own health with a comprehensive and short
instrument (6). The SF-36 has been validated
for use with older people, and its applicability
and suitability are well documented (5, 7, 8),
however, those versions cannot be used with
Iranian older people due to lack of cultural
equivalence. The existing Farsi SF-36 was translated
and validated for use with a general population
by an Iranian research team in 2005 (9), however,
it cannot be used directly with older people
owing to their heterogeneous characteristics
(6). There is also controversy surrounding the
numbers of underlying dimensions measured by
the different translated versions of the SF-36
compared to the US original SF-36 (10-12). Therefore,
a lack of a validated Farsi SF-36 for elderly
and controversy about the number of underlying
dimensions measured by the SF-36 highlights
the need to conduct a new psychometric analysis.
This study therefore investigates the factor
structure of the Farsi version of the SF-36
in older people to find the best-fitting model
for this population group.
Participants: A sample of 391 participants
(197 males and 194 females) were randomly selected
from the Tehran population and they ranged in
age from 60-89 years. The inclusion criteria
were age of 60 years and older and Abbreviated
Mental test score 6. The participants were asked
to complete the existing Farsi SF-36 (9), which
took about 20 to 30 minutes. The research was
approved by the ethics committee of the University
of Social Welfare and Rehabilitation Sciences
(USWR.REC.7393.162). Written informed consent
was obtained from each participant.
Instrument: The SF-36 Health Survey
assesses the mental and physical health status
and eight generic health concepts including
Physical Functioning (PF); Role Limitations
due to Physical Health (RP); Bodily Pain (BP);
General Health (GH); Vitality (VI); Social Functioning
(SF); Role limitations due to Emotional Health
(RE); and Mental Health (MH). The SF-36 has
been translated for use in several countries
as part of the International Quality of Life
Assessment (IQOLA) project (13, 14), and has
demonstrated reliability and validity across
diverse samples (3). The scale has 36 items
that are scored and summed according to a standardized
protocol and expressed as a score on a 0-100
scale for each of the eight health concepts,
with higher scores representing a better health
status (15). The psychometric testing of the
Farsi version of the SF-36 followed the procedure
of the IQOLA project (9).
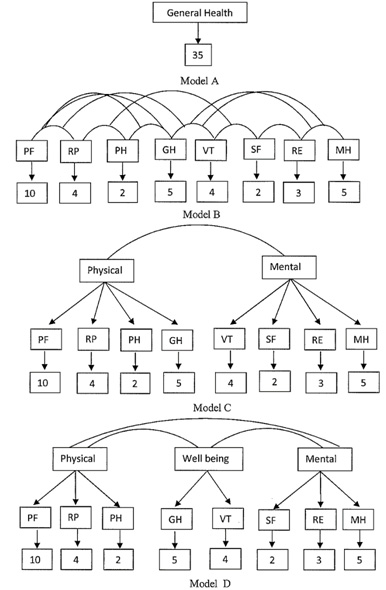
Data analysis: A confirmatory factor
analysis (CFA) on item level using LISREL 8.4
(16) assessed the fit and viability of the measurement
model which was developed from the original
US model (Model A) (15). The chi-square is significant
at p <.001 and an adequate fit is < 2.0.
The point estimate of the Root Mean Square Error
of Approximation (RMSEA) and its upper confidence
limit for the model should be less than 0.05
(17). The Expected Cross-Validation Index (ECVI)
(6.08) should be less than the ECVI for the
saturated model (3.23) (16). An exploratory
principal component analysis (PCA) was conducted
to explore the factor solution of the Farsi
SF-36 with both orthogonal and oblique rotations.
In this analysis, three alternative models were
examined to explore the best fitting model.
These alternative models were a one-factor model
(model B), a three uncorrelated second order
factor model (model C) based on previous studies
(18), and an eight-factor model (model D). Figure
1 depicts the diagrams of these three models
and the original US model (Model A).

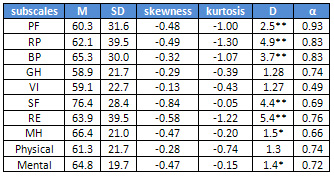
Descriptive
statistics
The
test
of
normality
of
the
scale
scores
showed
the
distributions
of
all
study
variables
were
negatively
skewed
(Table
1).
The
-coefficient
for
the
VI
was
very
low,
and
for
SF
and
MH
were
also
below
typically
accepted
standards.
On
the
other
hand,
Cronbach’s
alphas
were
adequate
for
the
GH,
RE,
Physical
and
Mental
components,
and
good
for
PF,
RP
and
BP.
Table
1:
Descriptive
statistics
and
K-S
test
of
normality
of
Persian
SF-36
scales
and
summary
measures
PF=
Physical
Functioning;
RP=Role-Physical;
BP=
Bodily
Pain;
GH=
General
Health;
VT=
Vitality;
SF=
Social
Functioning;
RE
=
Role-Emotion;
MH=
Mental
Health.
D
=
Kolmogorov-Smirnov
(K-S)
test
of
normality.
=
Cronbach’s
alpha.
**
P<.01.
*
P<.05
Testing
the
Sf-36
factor
structure
models
Four
CFA
models
were
developed
to
confirm
the
factor
structure
of
the
Farsi
SF-36.
This
analysis
served
to
confirm
Model
A,
the
original
US
model,
which
is
a
comparison
of
the
three
competing
models
to
ascertain
the
extent
to
which
the
Model
A
would
demonstrate
a
superior
fit
to
the
three
alternative
models.
Model
B,
the
first
alternative
model
was
developed
to
load
all
items
of
the
SF-36
into
a
single
health
construct.
The
second
alternative
model,
Model
C,
was
developed
from
the
three
summary
measures
of
mental,
physical
and
well-being
(18).
The
third
alternative
model,
Model
D
was
then
developed
based
on
the
eight
factors
that
aggregate
the
36
items
of
the
SF-36.
Table
2
indicates
how
Model
B
provided
a
poor
fit
for
this
data.
While
a
significantly
greater
model
fit
was
observed
for
the
original
US
model
(Model
A)
and
Model
C
and
D;
when
compared
to
Model
B,
these
models
did
not
demonstrate
a
good
fit.
Models
A,
C
and
D
however,
provided
a
relatively
better
fit
for
this
data.
An
examination
of
model
fit
statistics
revealed
mixed
evidence
for
a
good
model
fit,
where
all
models
did
not
fit
the
data
well,
according
to
the
significant
chi-square
index,
the
relative
chi-square
per
degrees
of
freedom
and
the
RMSEA
(17).
The
Comparative
goodness-of-fit
and
Incremental
Fit
Index
for
these
models
indicated
more
than
an
acceptable
model
fit,
but
the
goodness-of-fit
index
for
all
models
was
lower
than
the
accepted
criteria.
Together,
these
results
indicate
that
the
one-factor
did
not
provide
a
good
fit
for
this
data,
and
the
three
alternative
models
are
the
same,
according
to
the
fit
indices,
along
with
the
fact
that
their
overall
fit
did
not
appear
across
the
model
fit
statistics.
Table
2:
Factor
loadings,
communalities,
mean
and
standard
deviation
of
the
scales
of
the
Farsi
SF-36,
a
two
factor
solution
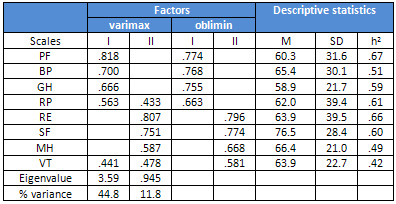
Note.
PF=
Physical
Functioning;
BP=
Bodily
Pain;
GH=
General
Health;
RP=Role-Physical;
RE
=
Role-Emotion;
SF=
Social
Functioning,
MH=
Mental
Health,
VT=
Vitality.
h2=
communality.
Factor
loading
>
0.4.
Cross-loaded
items
>
0.4.
Farsi
SF-36
factor
structure
A
PCA
of
the
eight
scales
was
conducted
with
orthogonal
and
oblique
rotations
to
explore
the
factor
structure
of
the
Farsi
SF-36,
and
examined
how
many
summary
measures
were
extracted
in
the
Iranian
sample.
The
analyses
demonstrated
only
one
factor
could
be
extracted
with
eigenvalues
over
1,
and
explained
a
total
44.9%
of
the
observed
variance.
The
original
two
measure
model
and
the
three
uncorrelated
measures
were
examined
and
a
scree-test
was
used
to
determine
the
proper
number
of
several
factor
solutions.
The
results
showed
that
the
first
two
factors
represented
the
main
sources
of
variance
in
the
data
matrix.
However,
the
results
of
orthogonal
rotation
showed
the
RP
and
VT
had
high
factor
loadings
on
both
factors.
The
results
of
the
oblimin
rotation
however,
showed
a
better
fit
of
the
original
measurement
model
because
all
eight
scales
were
loaded
on
their
appropriate
factors.
The
explained
variance
by
the
two
extracted
factors
was
56.7%.
The
communality,
eigenvalues
and
factor
loadings
for
the
two
rotated
factors
using
varimax
and
oblimin
rotations
are
presented
in
Table
2,
along
with
the
means,
and
standard
deviations
for
all
eight
scales.
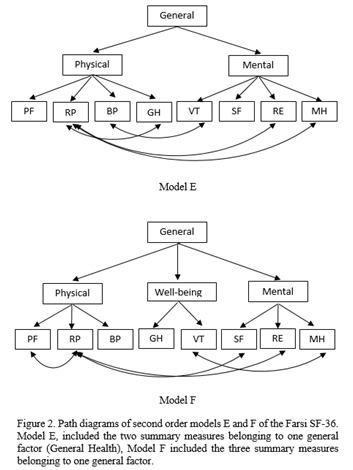
One
General
Health
Construct
A
second
order
CFA
based
on
the
two
factor
model
(Physical
and
Mental)
and
three
factor
model
of
adding
General
well-being,
were
loaded
on
a
one
general
health
conception.
This
analysis
served
to
explore
and
determine
the
underlying
latent
trait
in
the
SF-36
that
aggregates
the
summary
measures
(Figure
2).
Table
3
shows
how
both
models
demonstrated
an
unacceptable
fit
of
this
data.
The
chi
squares
were
significant,
with
p
<
0.05,
the
relative
chi
square
was
higher
than
2,
and
the
RMSEA
was
higher
than
0.05.
However,
the
goodness-of
fit
indices
were
acceptable
and
confirmed
both
models.
Click
here
for
Table
3:
The
Goodness
of
Fit
Statistics
for
CFA
Modified
and
non-modified
two
and
three
summary
measure
models
of
the
Farsi
SF-36
Note:
Model
E
included
the
two
summary
measures
belonging
to
one
general
factor
(General
Health),
Model
F
included
the
three
summary
measures
belonging
to
one
general
factor.
CFI=
Comparative
Fit
Index,
GFI=goodness
of
fit
index,
IFI=
Incremental
Fit
Index,
NFI=
Non
Normed
Fit
Index,
RMSEA=Root
Mean
Square
Error
of
Approximation,
ECVI=
Expected
Cross-Validation
Index.
ECVI
for
Saturated
Model=0.18.
*
P<
.05.
**
P<
.001
One
strategy
to
improve
the
models
was
to
add
the
correlations
between
error
terms
which
were
specified,
when
suggested,
by
high
modification
indices
and
also
where
theoretically
defensible.
In
Model
E,
the
correlated
errors
were
added
between
RP
items
with
GH,
RE
and
MH,
and
between
BP-VT.
The
correlated
errors
in
model
F
were
added
between
RP
with
PF,
SF,
RE
and
MH,
and
between
MH-VT.
An
examination
of
model
fit
statistics
after
modification
revealed
adequate
evidence
for
a
good
model
fit.
However,
in
both
Models
the
RP
scale
had
the
most
error
correlations
with
the
other
scales,
but
its
pattern
of
correlated
errors
was
different
in
the
models
with
GH,
RE
and
MH.
A
comparative
approach
of
the
four
factor
structure
models
of
the
Farsi
SF-36
is
presented
here.
Reliability
The
Farsi
SF-36
has
shown
satisfactory
internal
consistency
reliability
(>0.70)
for
all
scales
except
VI,
SF
and
MH,
with
the
highest
value
for
PF.
Similar
results
for
PF
have
been
reported
in
other
countries
(19),
which
was
to
be
expected
given
that
the
PF
scale
has
10
out
of
36
items
of
the
SF-36.
Such
a
large
set
of
items
increases
the
Cronbach’s
.
A
very
low
level
of
reliability
has
been
reported
for
the
VI
in
other
studies
conducted
with
older
people
and
patients
with
chronic
conditions
(10,
20,
21).
These
studies
determined
whether
the
lower
internal
consistency
of
the
SF-36
VI
scale
is
due
to
the
study
sample
or
cultural
differences,
although
this
deserves
further
study.
Additionally,
the
SF
scale
results
for
internal
consistency
reliability
were
below
typically
accepted
standards
in
Iran,
suggesting
a
decreased
level
of
social
abilities
among
older
adults.
The
fact
that
this
result
was
consistent
with
other
studies
(20,
22,
23)
raises
the
question
of
whether
only
two
items
in
the
SF
scale
are
adequate
for
assessing
the
concept
of
social
functioning.
Factor
structure
Both
two
and
three
factor
models
were
confirmed
in
the
Iranian
older
population,
however
a
comparison
of
fit
indices
of
the
higher
order
two-factor
model,
Model
A
with
two
summary
measures,
and
higher
order
three
factor
model,
Model
C
with
three
summary
measures,
showed
no
differences
between
these
two
models.
This
result
means
it
is
not
possible
to
show
a
preferred
model
for
older
people
and
suggests
the
instrument
is
conceptually
equivalent
with
the
original
version.
However,
the
question
remains
about
how
many
scales
could
be
extracted
from
this
concept.
The
two
factor
model
(mental
and
physical)
showed
PF,
RP,
BP
and
GH
to
correlate
with
physical
health
component,
and
VI,
SF,
RE
and
MH
with
the
mental
dimension.
These
results
are
consistent
with
other
studies
(24)
and
confirmed
the
Farsi
SF-36
met
the
psychometric
standards
hypothesized
in
the
original
model
for
physical
and
mental
health.
The
results
of
testing
a
three
second-order
factor
are
consistent
with
the
study
conducted
across
nine
countries
(18)
and
Rasch
validation
of
the
SF-36
in
Korea
(25).
The
third
factor,
interpreted
as
general
well-being
in
this
data,
was
the
result
of
clustering
GH
and
VI,
as
in
previous
studies,
and
interpreted
for
the
mixed
factor
content
of
GH
and
VI
(18).
The
reason
for
such
a
divergent
result
between
this
and
previous
studies
that
confirmed
the
two-factor
model
may
be
the
difference
in
separating
elderly
from
the
other
population
group.
Another
reason
for
this
divergent
result
is
that
cultural
value
plays
a
role
in
the
interpretation
of
these
differences,
and
Iranian
elderly
tend
to
put
more
value
on
items
related
to
well-being
compared
with
other
population
groups
and
cultures.
Therefore
the
three-factor
model
makes
the
Farsi
SF-36
particularly
suitable
for
use
in
the
assessment
of
older
adults,
as
its
three
scales
make
it
more
appropriate
to
identify
older
people’s
needs.
Such
data
makes
it
possible
to
develop
a
more
precise
care
plan,
since
the
more
factors
indicate
a
greater
identification
of
the
underlying
latent
trait.
The
three
factor
model
will
be
achieved
by
slightly
modifying
items
on
the
VI
scale
and
developing
items
for
the
well-being
scale.
The
Farsi
SF-36
has
generally
accepted
psychometric
properties,
with
empirical
evidence
showing
that
developing
items
for
the
third
factor
of
well-being
would
be
useful
to
better
identify
the
needs
of
older
people.
Acknowledgement
The
authors
of
this
paper
acknowledge
their
gratitude
to
Dr
Emma
Caukill
and
all
of
the
participants
in
this
research
project.
1.
Myint
PK,
Smith
RD,
Luben
RN,
Surtees
PG,
Wainwright
NW,
Wareham
NJ,
et
al.
Lifestyle
behaviours
and
quality-adjusted
life
years
in
middle
and
older
age.
Age
and
ageing.
2011;40(5):589-95.
2.
Garratt
A,
Schmidt
L,
Mackintosh
A,
Fitzpatrick
R.
Quality
of
life
measurement:
bibliographic
study
of
patient
assessed
health
outcome
measures.
BMJ.
2002;324(7351):1417.
3.
McHorney
CA,
Ware
JE,
Jr.,
Raczek
AE.
The
MOS
36-Item
Short-Form
Health
Survey
(SF-36):
II.
Psychometric
and
clinical
tests
of
validity
in
measuring
physical
and
mental
health
constructs.
Medical
care.
1993;31(3):247-63.
4.
McHorney
CA,
Ware
JE,
Jr.,
Lu
JF,
Sherbourne
CD.
The
MOS
36-item
Short-Form
Health
Survey
(SF-36):
III.
Tests
of
data
quality,
scaling
assumptions,
and
reliability
across
diverse
patient
groups.
Medical
care.
1994;32(1):40-66.
5.
Mishra
GD,
Gale
CR,
Sayer
AA,
Cooper
C,
Dennison
EM,
Whalley
LJ,
et
al.
How
useful
are
the
SF-36
sub-scales
in
older
people?
Mokken
scaling
of
data
from
the
HALCyon
programme.
Quality
of
life
research
:
an
international
journal
of
quality
of
life
aspects
of
treatment,
care
and
rehabilitation.
2011;20(7):1005-10.
6.
Hazard
WR.
principles
of
geriatric
medicine
and
gerontology1999.
1387-403
p.
7.
Bohannon
RW,
DePasquale
L.
Physical
Functioning
Scale
of
the
Short-Form
(SF)
36:
Internal
Consistency
and
Validity
With
Older
Adults.
Journal
of
Geriatric
Physical
Therapy.
2010;33(1):16-8.
8.
Hill
R,
Mansour
E,
Valentijn
S,
Jolles
J,
van
Boxtel
M.
The
SF-36
as
a
precursory
measure
of
adaptive
functioning
in
normal
aging:
the
Maastricht
Aging
Study.
Aging
Clin
Exp
Res.
2010;22(5-6):433-9.
9.
Montazeri
A,
Goshtasebi
A,
Vahdaninia
M,
Gandek
B.
The
Short
Form
Health
Survey
(SF-36):
translation
and
validation
study
of
the
Iranian
version.
Quality
of
life
research
:
an
international
journal
of
quality
of
life
aspects
of
treatment,
care
and
rehabilitation.
2005;14(3):875-82.
10.
Meng
H,
King-Kallimanis
B,
Gum
A,
Wamsley
B.
Measurement
bias
of
the
SF-36
Health
Survey
in
older
adults
with
chronic
conditions.
Quality
of
Life
Research.
2013;22(9):2359-69.
11.
Bartsch
L,
Butterworth
P,
Byles
J,
Mitchell
P,
Shaw
J,
Anstey
K.
Examining
the
SF-36
in
an
older
population:
analysis
of
data
and
presentation
of
Australian
adult
reference
scores
from
the
Dynamic
Analyses
to
Optimise
Ageing
project.
Quality
of
Life
Research.
2011;20(8):1227-36.
12.
Ngo-Metzger
Q,
Sorkin
DH,
Mangione
CM,
Gandek
B,
Hays
RD.
Evaluating
the
SF-36
Health
Survey
in
Older
Vietnamese
Americans.
Journal
of
Aging
and
Health.
2008.
13.
Ware
JE,
Jr.,
Keller
SD,
Gandek
B,
Brazier
JE,
Sullivan
M.
Evaluating
translations
of
health
status
questionnaires.
Methods
from
the
IQOLA
project.
International
Quality
of
Life
Assessment.
International
journal
of
technology
assessment
in
health
care.
1995;11(3):525-51.
14.
Ware
JE,
Jr.,
Gandek
B.
Overview
of
the
SF-36
Health
Survey
and
the
International
Quality
of
Life
Assessment
Project.
Journal
of
clinical
epidemiology.
1998;51(11):903-12.
15.
Ware
JE
KM,
Keller
SD.
.
SF-36
Physical
and
Mental
Component
Summary
Measures—A
User’s
Manual.:
Boston:
The
Health
Institute;
1994.
16.
Joreskog
KG
SD.
Scientific
Software
2003.
Available
from:
http://www.ssicentral.com/.
17.
Hu
L-t,
Bentler
PM.
Cutoff
criteria
for
fit
indexes
in
covariance
structure
analysis:
Conventional
criteria
versus
new
alternatives.
Structural
Equation
Modeling.
1999;6(1):1-55.
18.
Keller
SD,
Ware
JE,
Jr.,
Bentler
PM,
Aaronson
NK,
Alonso
J,
Apolone
G,
et
al.
Use
of
structural
equation
modeling
to
test
the
construct
validity
of
the
SF-36
Health
Survey
in
ten
countries:
results
from
the
IQOLA
Project.
International
Quality
of
Life
Assessment.
Journal
of
clinical
epidemiology.
1998;51(11):1179-88.
19.
Ware
JE,
Jr.,
Gandek
B,
Kosinski
M,
Aaronson
NK,
Apolone
G,
Brazier
J,
et
al.
The
equivalence
of
SF-36
summary
health
scores
estimated
using
standard
and
country-specific
algorithms
in
10
countries:
results
from
the
IQOLA
Project.
International
Quality
of
Life
Assessment.
Journal
of
clinical
epidemiology.
1998;51(11):1167-70.
20.
ten
Klooster
PM,
Vonkeman
HE,
Taal
E,
Siemons
L,
Hendriks
L,
de
Jong
AJ,
et
al.
Performance
of
the
Dutch
SF-36
version
as
a
measure
of
health-related
quality
of
life
in
patients
with
rheumatoid
arthritis.
Health
and
quality
of
life
outcomes.
2013;11:77.
21.
Hoopman
R,
Terwee
CB,
Deville
W,
Knol
DL,
Aaronson
NK.
Evaluation
of
the
psychometric
properties
of
the
SF-36
health
survey
for
use
among
Turkish
and
Moroccan
ethnic
minority
populations
in
the
Netherlands.
Quality
of
life
research
:
international
journal
of
quality
of
life
aspects
of
treatment,
care
and
rehabilitation.
2009;18(6):753-64.
22.
Pappa
E,
Kontodimopoulos
N,
Niakas
D.
Validating
and
norming
of
the
Greek
SF-36
Health
Survey.
Quality
of
life
research
:
an
international
journal
of
quality
of
life
aspects
of
treatment,
care
and
rehabilitation.
2005;14(5):1433-8.
23.
Tseng
HM,
Lu
JF,
Gandek
B.
Cultural
issues
in
using
the
SF-36
Health
Survey
in
Asia:
results
from
Taiwan.
Health
and
quality
of
life
outcomes.
2003;1:72.
24.
Ware
JE,
Jr.,
Kosinski
M,
Gandek
B,
Aaronson
NK,
Apolone
G,
Bech
P,
et
al.
The
factor
structure
of
the
SF-36
Health
Survey
in
10
countries:
results
from
the
IQOLA
Project.
International
Quality
of
Life
Assessment.
Journal
of
clinical
epidemiology.
1998;51(11):1159-65.
25.
Kim
SH,
So
WY.
Rasch
validation
of
the
SF-36
for
assessing
the
health
status
of
Korean
older
adults.
Journal
of
physical
therapy
science.
2015;27(3):601-6.
|
|
.................................................................................................................

|
| |
|
