Gender
Differences in Consultation Time and its Relation
to Patient's Satisfaction: a cross-sectional study
at King Khalid University Primary Health Care
Clinics In Riyadh, Saudi Arabia
Haya Al-Abbad
Correspondence:
Haya
Al-Abbad
Department: Family and Community Medicine
King Khalid University Hospital
Riyadh, Saudi Arabia.
P.O.BOX 5949, POSTAL CODE 11432
King Khalid university hospital, Family and
Community Medicine
Phone: 00966553163105
Email: Haya_alabbad@hotmail.com
|
Abstract
Background: Patient's
satisfaction is regarded as an outcome
of care in itself and is one of the major
contributors toward better patient compliance
leading, presumably, to better clinical
outcomes. Many studies have been done
in Saudi Arabia assessing health care
services but only few were conducted assessing
consultation per se and was quite a long
time ago. The objective of the study is
to find the relation between consultation
time and patient's satisfaction of both
male and female patients and the other
correlates of patient's satisfaction among
those attending Primary Health Care Clinics.
Methods: A
descriptive cross-sectional study was
carried out over April-June during 2013;
adult patients > 18 years old
were selected from Primary Care Clinics
in Riyadh City. Data was collected using
a self-administered questionnaire with
21 items of patient satisfaction scale.
Data were analyzed using descriptive and
analytic statistics.
Results: The
study included 400 patients. The average
consultation time among females was (16.28±8.006)
minutes and among males was (17.68±9.049)
with no significant difference (p-value=0.102,CI
-0.280,3.080). The mean satisfaction score
among females was (94.18,SD=±1.54),
while among males was (104.68,SD=±11.99).
The difference between the two groups
in the overall satisfaction score is significant.
Female patient's satisfaction was positively
correlated with consultation time as well
as the age. Among males, the satisfaction
didn't show any correlation with the consultation
time but it was negatively correlated
with marital status, experiencing bad
experience with family medicine doctor
in the last year, and with the waiting
time in waiting area.
Conclusion: Females'
satisfaction is positively correlated
with consultation time, with consideration
to give more time to them, focusing on
psychological problems, which needs better
doctor-patient communication skills. On
the other hand, males' satisfaction didn't
show significant correlation with consultation
time and other aspects of satisfaction
other than consultation itself should
be analyzed such as health care system
and services (waiting area setting, nurses,
pharmacy, and building).
Key words:
Consultation time, consultation length,
gender, patient satisfaction.
|
Patient satisfaction is regarded as an outcome
of care in itself and is one of the major contributors
toward better patient compliance leading, presumably,
to better clinical outcomes [1]. Through consultation,
one can measure the quality of care provided
and overall patient's satisfaction [2].
Many Studies have been conducted to assess patient's
satisfaction, most of them were about health
care services, others about drugs and prescriptions
[2, 3, 4, 5, 6] and few were about consultation
itself and consultation time. One study conducted
in Philadelphia, United States , reported mean
patient satisfaction with primary care physicians
of (62.9) for males and (60.7) for females [7].
Another study in Slovenia, reported that (58.2%)
of participants rated the level of care received
as excellent with no discrimination between
genders [1].
One study conducted at Ministry of Health facilities
in Jeddah, Saudi Arabia, assessed the factors
associated with patient's care during consultation
in 1997, and showed that the rate of patient's
satisfaction with the primary health care clinics
was (73.2%) without discrimination between genders
although the study stated that gender is a significant
factor affecting patient care [2]. Another study
conducted in Qateef, Saudi Arabia, assessed
the determinants of users' satisfaction with
primary health care settings in 1999 and included
consultation time as one the components, and
revealed the rate of patients' satisfaction
with consultation time as (79.7%) but again
no differences were shown between genders [4].
Many factors play a role on patient's satisfaction
during the consultation, including physician's
characteristics, patient's characteristics,
organizational factors and health care system
[8]. Among patients' characteristics, studies
found that gender difference has an effect on
patient's overall satisfaction [3]. Al-Dawood
mentioned that female gender is the most influential
factor [5] and some studies showed that females
are less satisfied with their consultation [3].
This in turn may be related to consultation
time, which could be short or insufficient for
them [9] and ultimately can affect patient's
satisfaction as was mentioned by Raja Lexshimi
who revealed low patient's satisfaction with
consultation time [10].
Hence, looking at consultation time, different
countries showed different average consultation
times [9, 11]. A study done in Europe measuring
consultation length among six different countries,
showed that Germany had the shortest consultation
time with mean of (7.6) minutes and Switzerland
had the longest consultation time with mean
of (15.6) minutes [9]. Another study in Qatar
stated that the mean time was (10.7) minutes
and for Arabian Gulf Areas was (5.9) minutes
[11 ]. In Saudi Arabia, a study was conducted
in eastern province primary health care centers
and showed that the mean consultation time was
(7.3) minutes with a range between (4.6-12.6)
minutes with no differences given between males
and females [5].
Different reasons attribute toward different
consultation times and ultimately to different
satisfaction rates. Female gender with their
own characteristics as they reported higher
psychological problems than males including
depression, anxiety and emotional issues [12],
had longer consultation time and the longest
consultation time was found when a female doctor
was dealing with a female patient [13].
Female gender needs longer consultation [2].
This study aims to identify if female patients,
in comparison with males, are satisfied with
longer consultation time at King Khalid University
Primary Health Care Clinics.
The rationale of this project is that many studies
have been done in Saudi Arabia assessing health
care services but only one was found that conducted
assessing consultation per se and was done in
1997 which is quite a long time ago. In fact,
satisfaction is one of the measures of quality
outcome, which needs to be assessed continuously.
This is a cross-sectional
study conducted from April-June,
2013 at Primary Health
Care Clinics in Riyadh,
Saudi Arabia. A total
of 400 patients (200 males,
200 females) were included
in the study. The sample
size was calculated based
on the assumption that
females are at twice the
risk of low satisfaction
than males, taking into
account CI=95% , power
of 80, ratio between male
and female =1 and percent
of control exposed =30%
with refusal rate of 10%.
Separate primary health
care clinics (PHCC) are
conducted for males and
females. Four (PHCC) were
randomly selected during
each morning and afternoon
slots (2 female and 2
male clinics ) and patients
were selected consecutively.
Male and female patients
attending PHCC >
18 years old were included
involving Saudi and non-Saudi
patients. These clinics
were run by Saudi and
non-Saudi doctors who
are working as (professors,
consultants, senior registrars,
registrars). Clinics that
were run by residents
and under graduate students
were excluded as well
as patients < 18 years
old, very ill patients
presenting as emergency
cases, and mentally retarded,
blind and deaf patients.
Data was collected through
self-administered questionnaire
from the period (April-June)
during 2013. Each questionnaire
had two parts; one for
the health care provider
with consultation time
and information about
the doctor, whereas the
second part was for the
patient. Patients were
asked to fill in the questionnaire
in the waiting area after
they were done with their
consultation. Written
and signed consent was
taken before filling in
the forms . One male and
female research assistants
were trained to collect
data and interview those
patients who had difficulty
in reading or writing.
Patients completed a questionnaire
consisting of Sociodemographic
characteristics (age,
gender, nationality, marital
status, educational level,
occupation, residence.
In cases if the participant
was married, educational
level and occupation of
the spouse was also inquired
about), health status
and factors related to
patient's satisfaction
(participants were asked
if they have any common
chronic diseases, any
history of stressors in
the last 6 months, a history
of bad experience with
family medicine doctor,
their next follow-up appointment,
waiting time in the waiting
area and things to be
changed if it was not
comfortable), and the
overall patient's satisfaction
scale (Medical Interview
Satisfaction Scale MISS-21).
MISS-21 consists of 21
items with four factors
(distress relief, communication
comfort, rapport and compliance
intent) with 7 point Likert
scale [1=very strongly
disagree,2=strongly disagree,3=disagree,4=uncertain,5=agree,6=strongly
agree,7=very strongly
agree]. The original scale
was validated, used and
adapted for British general
practice in 2002. The
scale was translated from
English to Arabic language
with backward translation
by two bilingual experts
(family physicians) as
no previous Arabic version
of the scale was found.
The minimum score is 21
and maximum score is 147.
The score used doesn't
have any cutoff point;
it is taken as a continuous
variable, the more the
score, the more the satisfaction.
Pilot testing was carried
out on 20 patients. Any
ambiguity identified was
removed with the approval
of an expert epidemiologist.
In addition, health care
providers completed a
questionnaire consisting
of doctor's gender, doctor's
nationality, professional
status, presenting problem
if new or follow up, and
the number of the visits
to the clinic within the
last 2 years. The consultation
time was calculated in
minutes by the health
care provider using her/his
watch from the moment
the patient entered the
room to the moment he/she
left. After collecting
the data, it was coded
and entered using SPSS
statistical software version
16. Descriptive statistics
were done. Frequency tables
and appropriate charts
of different variables
were performed. For seven
point satisfaction questions,
total score for each patient
was summated for all 21
questions. Maximum possible
score was (21*7=147).
To evaluate statistical
difference, Student-t
test was used for comparison
between mean values of
2 groups. Linear and multiple
regression analysis was
used to assess correlation.
P-value of < 0.05 was
used as a level of significance.
Approval was taken from
the departement administration.
Written consent was obtained
from those accepted to
participate. The survey
was anonymous and participants'
anonymity was assured
by assigning each questionnaire
with a code number for
the purposes of analysis
only.
Data
were
obtained
from
400
patients
giving
a
response
rate
of
89%.
The
sample
was
composed
of
200
females
and
200
males.
Mean
age
(SD)
of
female
patients
was
(43,
±14.37)
years
and
ranging
from
(>18
to
85)
years.
Mean
age
(SD)
of
males
was
(48,
±16.89)
years
and
ranging
from
(>18
to
86)
years.
The
difference
between
the
two
genders
in
age
is
significant
with
(p-value=0.002,
CI
=1.764-7.983).
Female
patients
represent
(99.5%)
Saudi
and
(0.5%)
non-Saudi
females,
whereas
male
data
represent
(95.5%)
of
the
sample
as
Saudi
and
(4.5%)
non-Saudi.
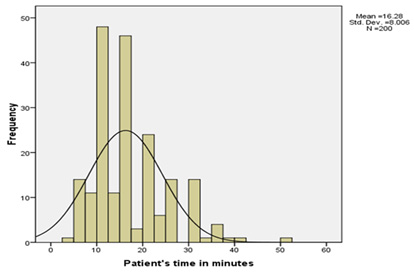
Average
consultation
time
among
females
was
(16.28)
minutes
(SD=8.006),
(minimum=4
minutes,
maximum=50
minutes).
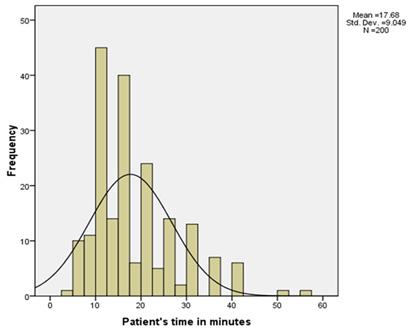
While
average
consultation
time
among
males
was
(17.68)
minutes
(SD=9.049),
(minimum=3
minutes,
maximum=55).
The
difference
between
the
two
groups
is
not
statistically
significant
with
(p-value=
0.102,
CI
=-0.280,
3.080)
as
shown
in
Table
1
and
Figures
1
&
2.
Table
1.
Average
consultation
time
of
both
genders:

Figure
1.
Frequencies
of
consultation
time
among
female
patients
Figure
2.
Frequencies
of
consultation
time
among
male
patients
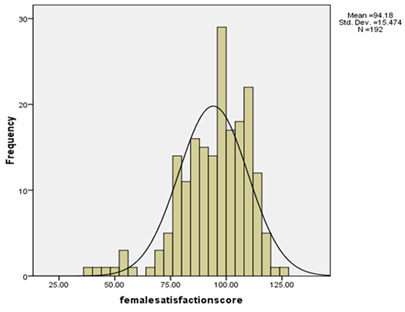
The
mean
satisfaction
score
among
females
was
(94.18±1.54).
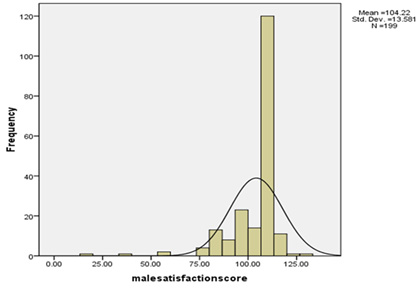
While
mean
satisfaction
score
among
males
was
(104.68±11.99).
The
difference
between
the
two
groups
in
the
overall
satisfaction
score
is
significant
with
(p-value=0.000,
CI=
7.139,12.947)
as
shown
in
Table
2
and
Figures
3
&
4.
Table
2.
Mean
satisfaction
scores
of
both
genders:

Figure
3.
Frequencies
of
overall
satisfaction
among
female
patients
Figure
4.
Frequencies
of
overall
satisfaction
among
male
patients
The
majority
of
female
patients
were
married
(64.5%)
as
were
male
patients
(85%).
For
education,
females
reported
that
most
of
them
were
at
the
level
of
high
school
(31%)
and
most
of
male
patients
were
at
the
level
of
university
and
advanced
studies
(42%).
For
occupation,
the
majority
of
female
patients
were
retired
or
housewives
(78.5%)
and
the
remaining
(21.5%)
were
either
students,
teachers
or
working
in
private
sector.
In
contrast,
most
of
male
patients
were
working
(60.1%)
while
(30.3%)
are
retired
and
(9.6%)
were
students.
The
majority
of
female
and
male
patients
were
coming
from
urban
rather
than
rural
areas
with
frequencies
of
(90.5%
vs.
9.5%)
respectively
for
both
genders.
The
main
reason
for
most
patients'
presentation
were
for
follow-up
and
old
problem
instead
of
new
problem
which
was
(87.%
vs.
12.%
)
respectively
among
females
and
(85%
vs.
15%)
among
males.
Chronic
diseases
have
been
reported
being
diagnosed
in
(82%)
of
females
(in
the
form
of
diabetes,
hypertension,
dyslipedemia,
osteoarthritis,
hypothyroidism,
depression,
bronchial
asthma,
obesity
or
other
diseases
such
as
cardiac,
renal,
gastritis
or
dermatological)
and
most
of
them
had
two
to
three
chronic
diseases
(34.5%)
whereas
among
males,
(97%)
reported
having
chronic
diseases
and
most
of
them
had
one
form
of
chronic
disease
(61%).
Most
female
patients
were
given
a
follow-up
appointment
within
6
months-<1
year
(66.5%)
whereas
male
patients
were
mostly
given
appointments
within
3-<6
months
(52.5%).
The
majority
of
the
patients
were
visiting
primary
health
care
clinics
more
than
twice
per
year
in
the
previous
two
years
(52.2%
and
43.3%)
among
female
and
male
patients
respectively.
Among
female
patients,
(43%)
reported
having
stressors
in
the
last
6
months
with
the
highest
stressors
being
socially
related
(40.69%
were
social,
26.9%
were
bereavement,
15.11%
were
financial,
9.3%
were
work-related,
9.3%
were
medical
and
4.6%
didn't
mention
the
type
of
their
stressors)
in
contrast,
(5.5%)
males
reported
having
stressors
(36.37%
reported
bereavement,
18.8%
reported
medical
stressors
and
45.45%
didn't
mention
their
type
of
stressor)
and
both
genders
fell
in
the
category
of
having
one
type
of
stressor
rather
than
having
multiple
stressors
within
the
last
6
months.
Reporting
bad
experience
was
mentioned
by
(5%)
of
females
and
(10.5%)
of
males
with
the
highest
bad
experience
for
females
being
in
communication
with
their
doctors
(40%)
but
for
males
(95%)
didn't
mention
what
type
of
bad
experience
they
had.
For
waiting
time
in
waiting
area,
females
showed
variable
frequencies
of
waiting
time
(19.5%
waited
5-<15
minutes,
24%
waited
15-<30
minutes,
28%
waited
30
minutes<1
hour
and
28%
waited
from
1-2
hours)
in
contrast,
for
males
(41%
waited
5-<15
minutes,
33%
waited
15-<30
minutes,
19.5%
waited
30-<1
hour
and
6.5%
1-2
hours).
When
reporting
about
if
the
waiting
area
was
comfortable
for
them,
(90.5%)
of
females
reported
that
it
was
comfortable
and
(77.5%)
of
males
reported
so.
Females
mentioned
that
the
things
that
must
be
changed
in
waiting
area
if
it
wasn't
comfortable
for
them
were
(100%
for
prayer
rooms,
63.15%
for
chairs,
47.36%
for
space
of
waiting
area,
36.84%
for
educational
aids,
36.48%
for
availability
of
bathrooms,
31.57%
for
privacy,
10.52%
for
cleanliness
and
26.31%
mentioned
other
things
such
as
receptionist.
While
males
showed
that
(53.3%
for
space
of
waiting
area
followed
by
40%
for
receptionist,
33.3%
for
availability
of
bathrooms,
26.6%
for
chairs,
11.11%
for
educational
aids,
8.88%
for
prayer
rooms
and
46.66%
didn't
mention
anything).
Female
patients
were
seen
by
female
doctors
most
of
the
time
(93.2%
seen
by
females
doctors
vs.
6.8%
seen
by
male
doctors)
as
did
males
where
they
were
seen
most
of
the
time
by
male
doctors
(93.5%
by
male
doctors
vs.
6.5%
seen
by
females).
For
professional
status
of
the
doctors,
(50.5%)
females
and
(54.5%)
males
were
seen
by
professor
or
consultant.
Most
of
females
and
male
patients
were
seen
by
Saudi
doctors.
The
majority
of
patients
were
seen
by
Saudi
doctors
(66.5%
of
females
vs.
54%
for
males).
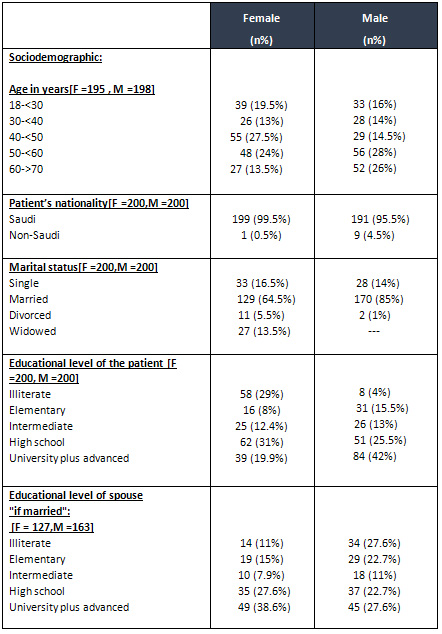
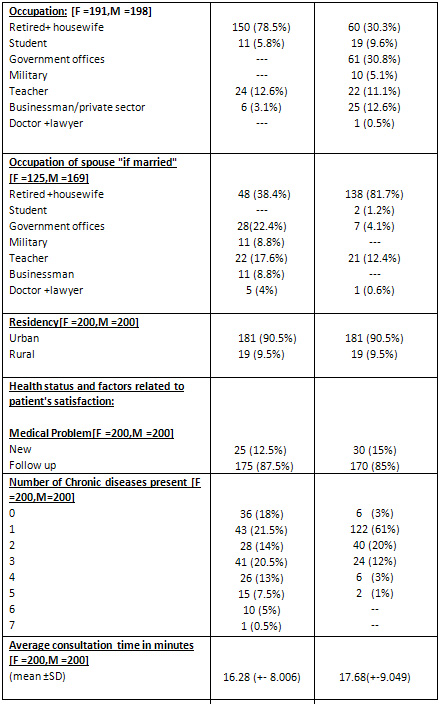
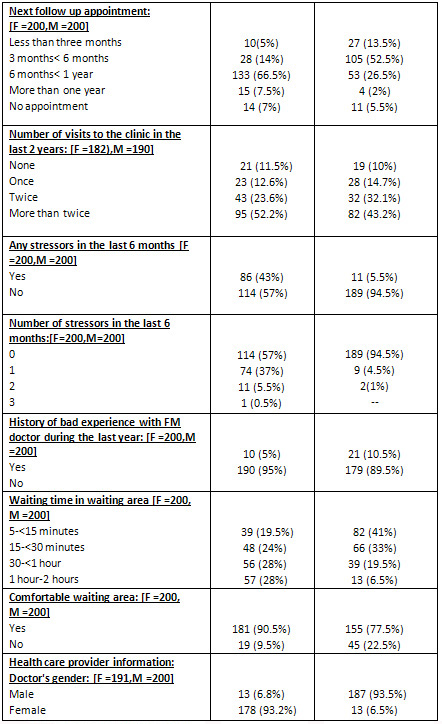
Table
3
shows
frequency
distribution
of
each
variable.
Separate
models
were
made
for
males
and
females.
Univariate
analysis
of
female
patients'
satisfaction
was
highly
significant
and
positively
correlates
with
the
consultation
time
(p-value
=0.003,
beta=0.211,
CI=
0.135,
0.668)
and
was
significant
with
positive
correlation
with
the
age
of
the
patient
(p-value=
0.009,
beta=0.190,
CI
=0.049,0.343).
It
didn't
show
any
correlation
with
other
sociodemographic
characteristics
or
other
related
factors
shown
in
Table
4.
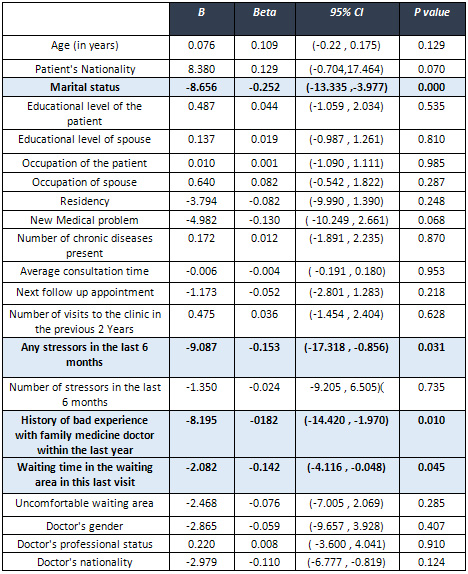
In
contrast,
male
patients'
satisfaction
didn't
show
any
association
with
the
consultation
time
(p-value=
0.952,
Beta=-0.004,
CI=
-0.191,0.180).
The
satisfaction
showed
negative
correlation
with
marital
status
(p-value=
0.000,
Beta=-0.252,
CI=
-13.335,-3.977),
presence
of
stressors
within
the
last
6
months
(p-value=
0.031,Beta=-0.143,
CI=
-17.318,-0.856),
history
of
bad
experience
with
family
medicine
doctor
within
the
last
year
(p-value
0.010,
Beta=-0.182,
C=I
-14.420,-1.970)
and
with
waiting
time
in
waiting
area
(p-value=
0.045,
Beta=-0.142,
CI=
-4.116,-0.048).
It
didn't
show
any
correlation
with
other
sociodemographic
characteristics
or
with
other
factors
related
to
patient's
satisfaction
as
shown
in
Table
5.
Table
3.
Descriptive
frequencies
of
sociodemographic,
health
care
provider
and
patient's
satisfaction
related
variables:
Table
4.
Univariate
analysis
of
female
patients'
satisfaction
score
with
sociodemographic,
health
status
and
health
care
provider
variables:
Table
5.
Univariate
analysis
of
male
patients'
satisfaction
score
with
sociodemographic,
health
status
and
health
care
provider
variables:
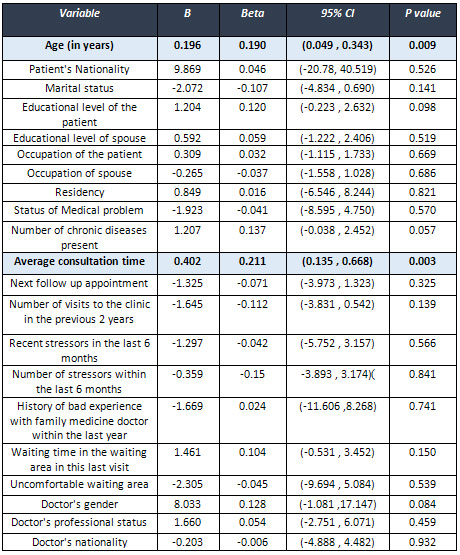
Multivariate
regression
showed
that
female
patient's
satisfaction
was
positively
correlated
with
only
consultation
time
(p-value=0.019,
Beta=0.176
,
CI=
0.054
,
0.588)
as
well
as
their
age
(p-value=
0.057,
Beta=
0.141
,
CI=
-0.005
,
-0.297).
Among
males,
the
satisfaction
didn't
show
any
correlation
with
the
consultation
time
(p-value=
0.869,
Beta=
0.011,
CI=-0.187,
0.221)
but
it
was
negatively
correlated
with
marital
status
(p-value=
0.000
,
Beta=
-0.243,
CI=
-12.992
,
-3.728),
experiencing
bad
experience
with
family
medicine
doctor
in
the
last
year
(p-value=0.009,
Beta=
-0.179,
CI=
-14.123
,
-1.997)
and
with
the
waiting
time
in
waiting
area
(p-value=0.033
,
Beta=
-0.146,
CI=
-4.098
,
-0.176)
as
shown
in
Tables
6
&
7.
Table
6.
Multivariate
analysis
of
female
patients'
satisfaction
score:
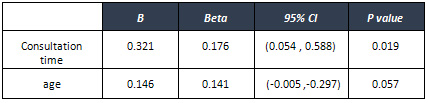
*The
results
were
adjusted
for
education
level,
occupation,
marital
status,
waiting
time
in
waiting
area,
number
of
chronic
diseases,
presence
and
number
of
stressors
within
the
last
6
months
and
history
of
bad
experience
with
family
medicine
doctor.
Table
7.
Multivariate
analysis
of
male
patients'
satisfaction
score:
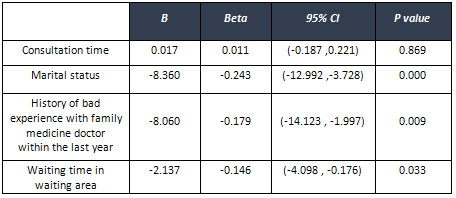
*The
results
were
adjusted
for
age,
education
level,
occupation,
number
of
chronic
diseases,
presence
and
number
of
stressors
within
the
last
6
months.
The
mean
consultation
time
of
female
patients'
(16.28±8.006)
minutes
and
of
males
(17.68
±9.049)
minutes
is
much
better
than
what
was
reported
earlier
from
PHCC
in
Saudi
Arabia.
One
study
conducted
at
eastern
province
showed
that
average
consultation
time
was
(7.3±5.7)
minutes
[5].
Another
study
conducted
in
Jeddah
reported
mean
consultation
time
of
(5.94±0.2)
minutes
[2].
Looking
at
different
aspects,
mean
consultation
time
for
Europe
was
(10.7±6.7)
minutes
with
the
longest
consultation
being
reported
in
Belgium
and
Switzerland
(15±7.2
and
15.6±8.7)
minutes
respectively,
whereas
in
Arabian
Gulf
countries,
the
average
consultation
time
was
(5.9±2.4)
minutes
[4].
This
improvement
in
consultation
time
would
reflect
the
improvement
in
the
health
care
system.
On
the
other
hand,
most
of
our
sample
patients
were
above
the
age
of
40
years.
Tahepold
H
reported
in
her
study
that
patients
>
46
years
of
age
had
longer
consultations
while
Myriam
Deveugele
mentioned
in
her
study
that
as
the
patient
age
increases
by
one
year,
the
consultation
time
increases
by
one
second
[9,
14
,
15
].
Most
of
the
patients
presenting
to
the
clinic
had
one
or
more
chronic
diseases
and
the
higher
the
number
of
health
problems,
the
more
the
consultation
time
[8].
Our
study
did
not
show
significant
difference
in
the
consultation
time
between
both
genders.
The
same
was
presented
in
a
study
conducted
at
an
Estonian
family
practice
[15].
The
studies
are
contradictory,
regarding
gender
and
consultation
time,
with
other
studies
showing
that
females
require
more
consultation
time
[
2,
9,
15].
Consultation
time
is
considered
one
of
the
main
factors
influencing
patient's
satisfaction
[16].
Looking
at
the
overall
patient's
satisfaction
first,
then
its
relation
with
consultation
time,
the
study
shows
that
the
score
of
patients'
satisfaction
of
both
genders
is
below
expected
with
significant
difference
between
female
and
male
patients
(
64.1%
for
females
vs.
71.2%
for
males)
(p.
value=0.00,
CI=7.139
,
12.947).
It
is
near
to
what
was
conducted
in
Jeddah,
which
reported
a
total
patient
satisfaction
of
both
genders
of
(73.2%)
[2].
Another
study
conducted
in
Qatar,
showed
satisfaction
rate
of
79%.
The
satisfaction
among
male
patients
is
higher
than
females.
Al-Dawood
identified
that
sex
of
respondents
is
the
most
influential
factor
on
the
level
of
satisfaction,
with
males
being
more
satisfied
[4].
Among
males,
consultation
time
didn't
show
an
association
with
the
level
of
satisfaction;
other
correlates
such
as
marital
status,
waiting
time
in
waiting
area
and
bad
experience
with
family
medicine
doctor
within
the
last
year
were
associated
with
it
inversely.
These
findings
were
also
shown
in
some
previous
studies.
Al-Faris
reported
that
being
married
is
associated
with
more
satisfaction
[4]
and
Hassali
reported
that
waiting
time
more
than
2
hours
is
associated
with
less
satisfaction
[16]
while
Janko
reported
from
a
study
conducted
in
Slovenia
that
waiting
in
waiting
room
has
the
poorest
satisfaction
[1].
Among
females,
satisfaction
score
positively
correlated
with
consultation
time.
The
more
time
given
to
females,
the
more
satisfaction.
Psychological
problems
and
stressors
tend
to
be
higher
among
females
and
the
presence
of
emotional
stressors
is
associated
with
less
satisfaction
as
mentioned
by
Jane
Odgen
[14].
Elaborating
on
psychological
stressors
takes
more
time
but
leads
to
better
satisfaction
especially
among
females.
In
our
study,
the
rate
of
psychological
problems
were
expected
to
be
higher
than
what
was
found.
Although
(10%)
of
females
reported
being
diagnosed
with
depression,
and
(43%)
reported
having
stressors
in
their
life
within
the
last
6
months,
they
didn't
show
an
association
with
patient
satisfaction.
This
could
be
explained
by
the
small
sample
of
patients
reporting
having
depression,
as
people
in
our
country
tend
to
be
conservative
with
some
cultural
barriers.
In
addition,
this
could
explain
the
overall
lesser
female
satisfaction
score.
Another
explanation
is
the
poor
communication
skills
rather
than
the
time
of
consultation
per
se.
Doctor-patient
communication
can
affect
rate
of
satisfaction
[3]
and
the
best
way
to
assess
this
is
by,
videotaping
the
consultation.
This
was
difficult
to
conduct,
as
it
is
culturally
not
accepted
by
Saudi
females.
Another
positive
correlate
for
female
satisfaction
in
this
study
is
the
age.
The
more
advanced
the
age,
the
more
is
the
satisfaction
which
is
in
accordance
with
the
findings
of
most
previous
studies
[3,
4].
Other
sociodemographic
factors
such
as
(level
of
education,
occupation
or
residency)
didn't
show
any
correlation
with
patients'
satisfaction
although
previous
studies
showed
less
satisfaction
with
lower
educational
level
or
being
unemployed
[4,
6].
Doctor
related
factors
such
as
gender,
nationality
or
professional
status
also
did
not
show
any
correlation.
C.
Carolyn
stated
that
physicians
can
promote
higher
satisfaction
by
the
way
they
interact
with
their
patients
[3]
and
with
perceived
empathy
from
the
doctors
[16].
Satisfaction
is
not
simply
a
product
of
patient
demographics
and
physician
skills,
it
is
also
affected
by
the
way
in
which
care
is
provided
[3].
It
is
a
complicated
construct
involving
an
array
of
factors
including
physician's
knowledge,
clinical
and
communication
skills,
accessibility,
convenience
and
location
of
surrounding
areas
and
continuity
of
care.
Female
satisfaction
is
positively
correlated
with
consultation
time,
with
consideration
to
give
more
time
to
them,
focusing
on
psychological
problems,
which
needs
better
doctor-patient
communication
skills.
On
the
other
hand,
males'
satisfaction
didn't
show
significant
correlation
with
consultation
time
and
other
aspects
of
satisfaction
other
than
consultation
itself
should
be
analyzed
such
as
health
care
system
and
services
(waiting
area
setting,
nurses,
pharmacy,
and
building).
The
study
highlights
the
need
to
increase
the
consultation
time
among
females
for
better
satisfaction
as
well
as
the
need
to
focus
on
psychological
problems
especially
among
females
with
good
training
in
communication
skills.
It
emphasizes
the
need
for
continuous
studies
for
evaluation
of
patients'
satisfaction
with
the
consultation.
Conducting
studies
for
evaluation
of
patients'
satisfaction
with
other
aspects
such
as
health
care
services
is
suggested,
since
they
play
a
major
role
in
overall
patients'
satisfaction.
This
study
had
some
limitation
in
the
form
of
study
sample
population.
Although
it
was
done
in
a
large
primary
care
clinic
in
Riyadh,
it
is
better
if
we
involve
other
primary
health
care
centers
in
Riyadh
to
make
the
generalization
more
accurate.
And
for
better
assessment
of
the
consultation
and
its
quality,
videotaping
should
be
used
but,
because
of
our
cultural
barriers
it
will
be
difficult
to
apply
with
a
high
rate
of
refusal
especially
among
females.
I
am
deeply
indebted
to
Dr.
Al-Johara
Al-Quiaz
(associate
professor
and
consultant
family
medicine
as
well
as
chair
of
princess
Nora
bint
Abdullah
for
women's
health)
and
Dr.Ambreen
Kazi
Kamran,
who
helped,
stimulated
suggestions
and
encouraged
me
in
all
the
time
of
research
work.
Apart
from
the
subject
of
my
research,
I
learnt
a
lot
from
them,
which
I
am
sure
will
be
useful
in
different
stages
of
my
life.
I'm
also
thankful
for
health
care
providers
and
colleagues,
who
helped
in
questionnaire
translation,
data
collection
and
data
entry.
1-Kersnik
J.
An
evaluation
of
patient
satisfaction
with
family
practice
care
in
Slovenia.
International
Journal
For
Quality
in
Health
Care.2000;
12(2):
143-147.
2-Balbaid
O,
Al-Dawood
K.
Factors
associated
with
patient's
care
during
consultation
in
ministry
of
health
facilities,
Jeddah
city,
Saudi
Arabia.
J
Family
Community
Med.
1997;
4(1):
46-52.
3-C.
Carolyn
Thiedke.
What
Do
We
Really
Know
About
Patient
Satisfaction?
Fam
Pract
Manag.
2007
;14(1):33-36.
4-Al
Qatari
G,
Haran
D.
Determinants
of
users'
satisfaction
with
primary
health
care
settings
and
services
in
Saudi
Arabia.
International
Journal
for
Quality
in
Health
Care.
1999
;
11(6):
523-531.
5-El-Mahalli
A,
Akl
O,
Al-Dawood
S,
Al-Nehab
A,
Al-Kubaish
H,
Al-Saeed
A,
Elkahky
A,
Salem
A.
WHO/INRUD
patient
care
and
facility-specific
drug
use
indicators
at
primary
health
care
centers
in
Eastern
province,
Saudi
Arabia.
Eastern
Mediterranean
Health
Journal.
2012
;18
(11):1086-1090
6-Saeed
A,
Mohammed
B,
Al-Doghaither
A.
Satisfaction
and
correlates
of
patients'
satisfaction
with
physicians'
services
in
primary
health
care
centers.
Saudi
Medical
Journal.
2001;
(3):262-267.
7-Hojat
M,
Louis
DZ,
Maxwell
K,
Markham
FW,
Wender
RC,
Gonnella
JS.
A
brief
instrument
to
measure
patients'
overall
satisfaction
with
primary
care
physicians.
Family
Medicine
Journal.
2011;43(6):412-7.
8-Ster
M,
Svab
I,
Kalan
G.
Factors
related
to
consultation
time:
Experience
in
Slovenia.
Scandinavian
Journal
of
Primary
Health
Care.
2008
;
26:
29-34.
9-Deveugele
M,
Derse
A,
Brink-Muinen
A,
Bensing
J,Maeseneeer
J.
Consultation
length
in
general
practice:
cross
sectional
study
in
six
European
countries.
BMJ.
2002;
325:472-477.
10-Lexshimi
R,
Zaleha
M,
Shamsul
A,
Suriawati
G.
Patient
satisfaction
on
waiting
time
and
duration
of
consultation
at
Orthopedic
Clinic,
Universiti
Kebangsaan
Malaysia
Medical
Centre.
Med
Health
Journal.
2009;4(1):35-46.
11-Bener
A,
Al-Marri
S,
Abdulaziz
A,
Ali
B,
Al-Jaber
K,
Mohammed
H.
Do
Minutes
Count
for
Health
Care?
Consultation.
Length
in
a
Tertiary
Care
Teaching
Hospital
and
in
General
Practice.
Middle
East
Journal
of
Family
Medicine.
2007;
5
(1).
12-Tabenkin
H,
Goodwin
E,
Zyzanski
S,
Stange
K,
Medalie
J.
Gender
Differences
in
Time
Spent
during
Direct
Observation
of
Doctor-Patient
Encounters.
Journal
of
Women's
Health.
2004;13
(3):341-349
13-Hutton
C,
Gunn
J.
Do
longer
consultations
improve
the
management
of
psychological
problems
in
general
practice?
A
systematic
literature
review.
BMC
Health
Services
Research.
2007;7(71).
14-Ogden
J,
Bavalia
K,
Bull
M,
Frankum
S,
Goldie
C,
Gosslau
M,
Jones
A,
Kumar
S
and
Vasant
K.
"I
want
more
time
with
my
doctor":
a
quantitative
study
of
time
and
the
consultation.
Family
Practice.
2004;
21(5):
479-483.
15-
Tähepold
H,
Maaroos
HI,
Kalda
R,
Brink-Muinen
A.
Structure
and
duration
of
consultations
in
Estonian
family
practice.
Scand
J
Prim
Health
Care.
2003;21(3):167-70.
16-Hassali
M,
Alrasheedy
A,
Razak
B,
ALtamimi
S,
Saleem
F,
Haq
N,
ALjadhey
H.
Assessment
of
general
public
satisfaction
with
public
healthcare
services
in
Kedah,
Malaysia.
Australian
Medical
Journal.
2014;
7(1):35-44.
17-Bertakis
K.
The
influence
of
gender
on
the
doctor-patient
interaction.
Patient
education
and
counseling.
2009
;76(3):356-360
18-Meakin
R,
Weinman
J
.The
'Medical
Interview
Satisfaction
Scale'
(MISS-21)
adapted
or
British
general
practice.
Family
Practice.
2002;19:257-263.
19-Howie
J,
Porter
A,
Heaney
D,
Hopton
J.
Long
to
Short
consultation
ratio:
a
proxy
measure
of
quality
of
care
for
general
practice.
British
Journal
of
General
Practice.
1991;41:48-54.
20-Fenton
J,
Jerant
A,
Bertakis
K,
Franks
P.
The
Cost
of
Satisfaction:
A
national
Study
of
Patient
Satisfaction,
Health
Care
Utilization,
Expenditures,
and
Mortality.
ARCH
Intern
Med.
2012
;172(5).
21-Abioye
EA,
Bello
IS,
Olaleye
TM,
Ayeni
IO,
Amedi
MI.
Determinants
of
patients
satisfaction
with
physician
interaction:
a
cross-sectional
survey
at
the
Obafemi
Awolowo
University
Health
Centre,
IIe-Ife,
Nigeria.
SA
Fam
Pract.
2010;52(6):557-562.
22-Baker
R.
Characteristics
of
practices,
general
practitioners
and
patients
related
to
levels
of
patients'
satisfaction
with
consultation.
British
Journal
of
General
Practice.
1996
;46
:
601-605.
|

