|
|
 |
Medicine and Society
........................................................
Clinical
Research and Methods
........................................................
|
Chief
Editor -
Abdulrazak
Abyad
MD, MPH, MBA, AGSF, AFCHSE
.........................................................
Editorial
Office -
Abyad Medical Center & Middle East Longevity
Institute
Azmi Street, Abdo Center,
PO BOX 618
Tripoli, Lebanon
Phone: (961) 6-443684
Fax: (961) 6-443685
Email:
aabyad@cyberia.net.lb
.........................................................
Publisher
-
Lesley
Pocock
medi+WORLD International
11 Colston Avenue,
Sherbrooke 3789
AUSTRALIA
Phone: +61 (3) 9005 9847
Fax: +61 (3) 9012 5857
Email:
lesleypocock@mediworld.com.au
.........................................................
Editorial
Enquiries -
abyad@cyberia.net.lb
.........................................................
Advertising
Enquiries -
lesleypocock@mediworld.com.au
.........................................................
While all
efforts have been made to ensure the accuracy
of the information in this journal, opinions
expressed are those of the authors and do not
necessarily reflect the views of The Publishers,
Editor or the Editorial Board. The publishers,
Editor and Editorial Board cannot be held responsible
for errors or any consequences arising from
the use of information contained in this journal;
or the views and opinions expressed. Publication
of any advertisements does not constitute any
endorsement by the Publishers and Editors of
the product advertised.
The contents
of this journal are copyright. Apart from any
fair dealing for purposes of private study,
research, criticism or review, as permitted
under the Australian Copyright Act, no part
of this program may be reproduced without the
permission of the publisher.
|
|
|
| March 2015 - Volume
13 Issue 2 |
|
The
Effectiveness of Hand Hygiene Education Intervention
for Medical Students in Primary Care Settings,
Ismailia City, Egypt
Hebatallah Nour-Eldein
(1)
Nahed Amen Eldahshan
(2)
(1) Assistant Professor of Family Medicine,
Suez Canal University,
Ismailia City, Egypt
(2) Lecturer of
Family Medicine, Suez Canal University,
Ismailia
City, Egypt
Correspondence:
Hebatallah Nour-Eldein, Assistant Professor
of Family Medicine,
Suez Canal University,
Ismailia
City, Egypt
Moblile:
01274079405
Email:
hebanour20@hotmail.com
|
Abstract
Background: All medical students
must be aware and practice hand hygiene
procedures as one of the infection control
measures that could lower health care
acquired infections.
Aims: to improve practice of hand
hygiene among medical students in health
care settings and to evaluate the effectiveness
of educational training on hand hygiene
among the medical students.
Methods: The study is a prospective
before-and-after trial of an educational
intervention with longitudinal follow
up. Pre-post intervention was between
April and May 2014 with one month interval
and the follow up was 6 months later.
The pre post intervention included all
the first year medical students with affiliation
to Faculty of medicine, Suez Canal University
in Ismailia city. The follow up included
all the participants who continued their
second educational year in the same faculty.
The researchers used a validated questionnaire
and observation checklist to collect data
in all periods of the study. Educational
training program was designed and conducted
by the researchers on hand hygiene importance,
measures, technique, time and compliance.
Results: The educational intervention
had a significant improvement in KAP,
one and six months after the intervention
(P <0.001). Non significant decrease
in median scores of knowledge with no
change in median scores of attitude but
significant improvement of median scores
of practice and overall KAP scores of
hand hygiene in the follow up (P <0.001)
was observed.
Conclusion: The educational intervention
was effective in improvement in KAP of
hand hygiene in pre-post intervention
with one month interval and in the follow
up after six months after the intervention.
Key words: Hand hygiene, intervention,
medical students
|
Hand hygiene is a general term referring to
any action of hand cleansing. The World Health
Organization (WHO) guidelines on hand hygiene
in health care provide a comprehensive review
of scientific data on hand hygiene rationale
and practices in health care. The strategy of
"My five moments for hand hygiene"
by WHO, can be used to ensure proper education
of the trainee health work force. These five
moments that call for the use of hand hygiene
include the moment before touching a patient,
before performing aseptic and clean procedures,
after being at risk of exposure to body fluids,
after touching a patient, and after touching
patient surroundings.[1]
Hand hygiene awareness and compliance among
undergraduate medical students of the Qassim
College of Medicine, Saudi Arabia, was very
low.[2] There was a previous study in Ain Shams
University hospitals in Cairo that recommended
the implementation of hand washing training
programs for undergraduate doctors, house officers
and nurses to improve Hand wash practice. [3]
Also in a study comparing hand hygiene knowledge,
beliefs and practices of Italian nursing and
medical students, mean scores on the knowledge
questions were low for both groups and in another
Italian study knowledge of the medical students
was lower than that of nursing students; also
they had lower values in adherence to practice.[4,5]
Students are bound to develop faulty hand hygiene
practice if the curriculum is not enforced with
hand hygiene concepts and skills.[2] Behavioral
change is part of hand hygiene intervention
and the dynamic of behavioral change is complex
and multifaceted. It involves a combination
of education, motivation, and system change.[1]
Education is pivotal to the outcome of effective
healthcare-associated training programmes and
nowhere is this more apparent than in infection
prevention and control (IPC). Hand hygiene is
one of the basic principles of ICP and requires
all healthcare practitioners (and others) to
consider IPC as an integral part of their lives
and working practice.[6] Previous studies have
revealed educational deficits among medical
students regarding patient safety. It has been
previously recommended that the importance of
hand hygiene must be taught to medical students
from the first year and integrated into their
clinical curriculum.[7,8]
The medical students in Faculty of medicine-Suez
Canal University are in direct contact with
patients from their first year of education
in primary care clinical training. This item
is not included in their family medicine theoretical
curriculum and is supposed to be learned during
their clinical training which could differ from
one to another primary care centers or trainers.
All primary care centers have policies and procedures
of infection control measures including hand
hygiene. All the medical students must be aware
and practice hand hygiene procedures as one
of the infection control measures that could
lower health care acquired infections.
To improve practices of
hand hygiene among medical
students in health care
settings and to evaluate
the effectiveness of educational
training on hand hygiene
among the medical students.
Design:
The study is a prospective
before-and-after trial
of an educational intervention
with longitudinal follow
up. Pre-post intervention
was carried out in 6
training primary care
units (4 urban and 2
rural settings) in Ismailia
city between April and
May 2014. The pre intervention
assessment and the educational
intervention were conducted
in April while the post
intervention was carried
out one month later.
Follow up was carried
out in the same primary
care units, 6 months
later between November
and December in the
first term of the second
educational year (2014-2015).
Participants:
The pre-post intervention
included all the first
year medical students
with affiliation to
Faculty of medicine,
Suez Canal University
in Ismailia city; 145
completed the intervention
out of a total 153 with
a response rate of 94.8%.
The follow up was carried
out among all the participants
who continued their
education in the same
faculty,132 out of total
137, with a response
rate of 96.4% as 16
participants moved from
the faculty of medicine
in Ismailia city to
Port Said city, 4 students
were recurrently absent
at the time of follow
up and one student recently
joined the second year
and was excluded.
Questionnaire:
A validated modified
questionnaire was self-administered
by the medical students
before and after their
clinical training on
hand hygiene and in
the follow up.
The questionnaire included
4 sections:
1. Characteristics
of the medical students;
training, if they had
been previously educated
about hand hygiene within
the primary care unit;
whether they previously
learned about hand hygiene
from the posters or
lectures.
2. Knowledge
of hand hygiene included:
source and main route
of transmission of harmful
germs, 5 moments of
hand hygiene; the precautions
with hand hygiene; the
difference between routine
hand wash with soap
and water and alcohol
based hand rub in indications,
time and their efficiency.
Knowledge test was previously
used among medical and
nursing students in
other studies.[9-11]
The selected items were
adapted from WHO's hand
hygiene questionnaire
for health care workers.[12]
It included multiple
choice and "false"
or "true"
questions. Maximum score
was 25.
3. Attitude was
assessed by 4 questions
that were developed
by the researchers including
the support with sufficient
knowledge; importance
of hand hygiene; their
readiness to practice
and the presence of
facilitation to use
it within primary care
units. They were given
a score three for agree,
two for not sure and
one for don't agree
with a maximum score
of 12.
4. Practice included
3 parts: compliance
(self report), technique
of hand wash including
hand rubbing steps and
its duration (observation).
Compliance was self-reported
in the questionnaire
as correct practice
of hand hygiene on physical
examination of their
last 3 patients; if
they practiced hand
hygiene before, after
or both. It scores one
to yes and zero to no
or sometimes. Maximum
score was 2 for before
and after. The students
who reported the correct
practice before and
after were considered
compliant. The questionnaire
was translated into
Arabic, then it was
back translated into
English by a bilingual
consultant; both translators
met for necessary modifications,
restatement and rewording.
A Pilot study was carried
out before the study
on a sample of students
to assess the feasibility
and reliability of the
questionnaire.
Observation checklist:
An observation checklist
was used to assess the
whole technique of hand
washing in eleven steps
(e.g. run water, use
soap, rubbing the palm
of the hand, rubbing
the dorsum of the hand,
rubbing between fingers,
rubbing the back of
fingers, rubbing the
thumbs, rubbing the
finger tops within the
palms, rinse the hands,
drying their hands and
closing tap with single
use towel). Time of
hand washing was also
assessed. WHO recommends
40-60 seconds for hand
washing with 20-30 seconds
of hand rubbing.[1,
12] Maximum score of
practice was 14: 2 for
compliance which was
added to 11 of hand
wash technique and 1
for the appropriate
time. Observations were
recorded by the first
author to avoid bias.
Maximum score of Knowledge,
attitude and practice
(KAP) was 51.
Training program:
It was conducted for
all the first year medical
students. It has a theoretical
and practical orientation.
Both were adapted from
WHO guidelines and the
monograph by the Joint
Commission 2009.[1,12]
The program lasted 90
minutes. It was structured
as follows:
1. Brief overview
of the background of
infection prevention
and WHO concept of five
moments for hand hygiene.
[1]
2. All students
were made aware of their
non-adherence to hand
hygiene, a strategy
aimed to enhance responsibility
awareness and behavioral
change.
3. Instructions
for optimal hand hygiene
procedures. These mainly
focused on the timing
and the whole technique
of hand washing.
4. Instructions
about the similarities
between the Alcohol
based hand rubbing and
the hand wash with water
and soap in involvement
of 6 areas for rubbing
with the difference
in indications, time,
drying and efficiency.
5. Performance
feedback on personal
hand hygiene practices
and peer auditing.
6. Tutors and
health care workers
within primary care
units and centers were
encouraged to improve
social norms regarding
hand hygiene by serving
as role models, encouraging
medical students to
comply with hand hygiene
protocol and building
a culture shift to better
hand hygiene.
Methods of training:
A lecture in 30 minutes
represented the theoretical
part; videos regarding
the WHO concept of technique
and five moments for
hand hygiene were presented
to them; along with
cluster-field training;
small group discussion;
simulations followed
by one-to-one teaching
method of hand washing.
Tutors were encouraged
to remind the student
to comply with hand
hygiene measures. At
every primary care unit:
each training clinic
had a washing sink,
liquid soap dispensers
and drying tissues.
Reminders in primary
care units: illustrative
posters of the steps
of hand wash were above
each sink. Reminders
on hand: printed figures
of hand hygiene and
the educational videos
were sent to the students
through their email.
Outcome measures:
Knowledge, attitude,
practice of hand hygiene
were assessed in pre-post
intervention and in
the follow up.
Ethical clearance:
The study was approved
by the ethics committee
of Faculty of Medicine,
Suez Canal University
(no.2086) and was performed
in accordance with the
ethical standards laid
down in the Declaration
of Helsinki (1964).
Informed consents were
obtained from medical
students who participated
in the study. Questionnaire
did not contain any
critical questions and
confidentiality of data
was maintained.
Statistical analysis:
The collected data were
analyzed using SPSS
20.0 for Windows. Categorical
data are presented as
numbers and percentages.
Continuous data as the
knowledge, attitude
and practice scores
and total scores before
and after the educational
intervention were tested
for normality of distribution
using one sample Kolmogorov-Smirnov
test. The samples were
found not to follow
a normal distribution
and median was calculated
as a measure of central
tendency, interquartile
range as measure of
variance. Non-parametric
tests were used for
comparison across the
different periods of
intervention. Friedman
two-way test for repeated
measures was used to
compare median values
in the three evaluations
and Wilcoxon signed
- rank test with post-hoc
correction in paired
measures for continuous
variables. Cochran Q
test was used for repeated
measures to assess changes
over time and McNemar
test for pairwise measures
when comparisons were
in categorical variables.
Median of knowledge,
attitude, practice and
total scores were compared
among different subgroups
of participants with
regard to characteristics
of the students: gender,
site of PHC, learning
and training of infection
control measures before
and after the intervention
using the Mann-Whitney
test for dichotomous
variables. A p value
less than 0.05 was taken
as statistically significant,
with post hoc Bonferroni
correction p value less
than 0.016 considered
statistically significant.
Spearman correlation
test was used to test
significant relationship
between knowledge attitude
and practices scores
in the different study
periods.
The
pre-post
intervention
sample
was
all
the
first
year
medical
students.
The
follow
up
were
in
the
second
medical
year.
The
mean
age
of
students
at
the
start
of
the
study
was
18.5±0.65.
More
than
half
of
the
study
sample
were
female
(57.9%).
More
than
two
thirds
of
the
study
sample
(71.7%)
were
trained
in
rural
PHC
units.
All
the
trainers
were
family
physicians.
No
previous
formal
training
in
the
PHC
units
was
experienced
by
most
of
the
students.
Previous
learning
was
mentioned
by
only
(13.8%)
of
the
sample.
Repeated
measures
of
knowledge,
attitude
and
practice
of
hand
hygiene:
The
intervention
leads
to
statistically
significant
change
between
the
pre,
post
intervention
and
follow
up
in
the
median
scores
of
knowledge
(14,
23,
22),
attitude
(8,11,11),
practice
(6,
11,13)
of
hand
wash
and
the
overall
KAP
scores
(28,
44,
46)
(P<0.001).
The
changes
in
median
scores
of
knowledge,
attitude,
practice
and
the
overall
KAP
were
statistically
significant
in
the
Pre-post
intervention
and
pre-follow
up
of
the
intervention.
In
post-follow
up
of
intervention,
statistically
significant
change
was
observed
in
the
median
scores
of
practice
and
the
overall
KAP
with
no
statistically
significant
change
in
median
scores
of
knowledge
or
attitude.
(Table
1)
Click
here
for
Table
1:
Comparison
of
pre,
post
intervention
and
follow
up
of
students'
knowledge,
attitude,
practice
and
total
KAP
of
hand
hygiene
(n=132)
Pre-post
intervention
changes
in
practice
of
hand
hygiene
Technique:
The
present
study
revealed
a
highly
statistically
significant
increase
in
practice
of
all
steps
of
hand
wash
among
the
study
sample
in
pre-post
intervention
with
maintenance/improvement
in
the
follow
up
after
6
months.
The
palms
and
backs
of
the
hands
were
more
frequently
observed
than
other
areas
of
hand
rubbing
among
pre-post
intervention
and
in
the
follow
up
(P
<
0.001).
[Table
2]
Click
here
for
Table
2:
Comparison
of
pre,
post
and
follow
up
of
students'
practice
sub-items
Time:
The
frequency
of
students
who
practiced
hand
rubbing
in
appropriate
time
increased
significantly
in
pre-post
intervention
from
(5.3-50.8%)
and
increased
in
the
follow
up
among
(69.7%)
of
the
students
(P
<
0.001).
[Table
2]
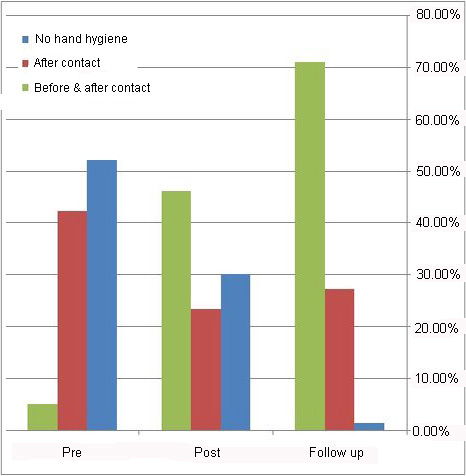
Compliance:
The
appropriate
practice
of
hand
hygiene
before
and
after
patient
contact
was
reported
by
only
(5.3%)
of
the
students
which
significantly
increased
to
(46.2%)
while
it
increased
among
(71.2%)
of
the
students
in
the
follow
up
(P<0.001).
[Table
2]
No
hand
wash
was
decreased
among
the
students
from
(52.3
to
30.3)
in
pre-post
intervention
with
further
decrease
to
(1.5%)
in
the
follow
up.
[Figure
1]
Figure
1:
Comparison
of
pre-post
intervention
and
follow
up
of
self
reported
compliance
of
hand
hygiene
Pre-post
changes
in
knowledge,
attitude,
and
practice
changes
and
personal
characteristics
of
the
study
sample:
There
was
a
high
statistically
significant
relationship
between
the
changes
in
knowledge,
attitude
and
practice
with
previous
training
and
the
greater
differences
were
observed
among
those
who
didn't
receive
training.
Correlations
between
Knowledge,
attitude
and
practice
across
the
study
periods
Statistically
significant
correlations
were
found
between
knowledge,
attitude
and
practice
scores
in
each
period
of
the
study.
[Table
3]
Table
3:
Correlation
between
Knowledge,
attitude,
practice
scores
among
the
study
sample
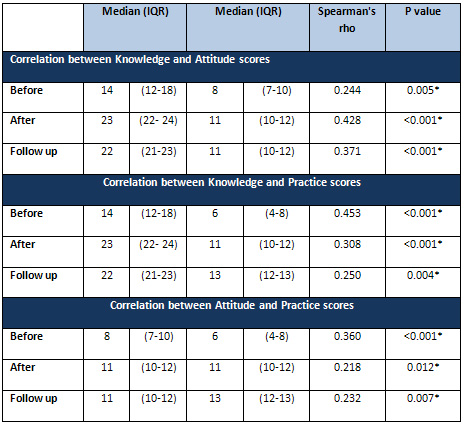
*
Bivariate
analysis
using
Spearman's
correlation
P
Value
<
0.05
The
intervention
was
effective
in
changing
the
knowledge,
attitude,
practice
and
overall
KAP
scores
among
the
students
in
all
periods
of
the
study
with
a
high
statistically
significant
difference
between
the
pre
intervention
and
the
follow
up.
The
non
significant
decrease
of
median
scores
of
knowledge
and
maintenance
in
median
scores
of
attitude
in
the
follow
up;
with
the
improvement
in
the
practice
and
overall
scores
of
practice
and
KAP
could
be
due
to
the
maintenance
of
the
same
situations
in
practice
settings
and
the
reminders
that
were
on
hand
of
the
students.
These
results
were
nearly
similar
to
the
results
in
a
quasi-experimental
study
among
100
randomly
assigned
nurses
to
receive
an
educational
intervention
prior
to
and
4
months
after
the
training.
The
educational
training
significantly
improved
Chinese
nurses'
knowledge,
practice,
and
behavior
related
to
universal
precautions
by
Huang
et
al.,
[13]
and
the
Iranian
study
by
Rezaee
et
al.,
[14]
on
4th
year
medical
students
as
a
significant
difference
were
found
between
the
pre
and
the
late
post-test
scores
in
knowledge
and
performance
but
not
the
attitude.
Also
they
found
a
significant
difference
only
in
the
performance
pre-test
and
immediate
post-test
scores,
category.
While
another
intervention
by
Gould
and
Chamberlain[15]
determined
the
effect
of
a
hand
hygiene
education
program
after
3
months
and
found
no
effect
of
the
program.
The
difference
could
be
related
to
the
difference
in
the
used
tools
of
assessment.
There
was
significant
increase
of
the
students
(40.2%)
that
correctly
rub
of
palm
to
palm
from
(59.8
to
100%)
with
maintenance
of
100%
in
follow
up.
Also
there
was
an
increase
in
palm
to
back
from
(50
to
100%)
without
change
in
the
follow
up.
Students
who
rub
between
fingers
were
increased
significantly
from
(28
to
81.8%)
with
increase
to
87.9%
in
the
follow
up.
Students
with
rubbing
of
the
back
of
fingers
were
increased
significantly
from
(16.7
to
62.9%)
with
increase
to
90.2%
among
the
students
in
the
follow
up.
Thumb
rubbing
was
increased
among
the
students
from
(22.7
to
81.1%)
with
increase
to
96.2%
of
the
students.
Rubbing
of
the
top
of
fingers
increased
from
(16.7
to
62.9%)
in
pre-post
intervention
with
increase
to
87.1%
in
the
follow
up.
These
results
were
similar
to
those
of
Helder
et
al.,[16]
who
found
that
along
all
observation
periods
the
palms
and
backs
of
the
hands
were
significant
better
disinfected
than
wrists,
between
fingers,
finger
tops
and
thumbs.
Regarding
the
reported
compliance
of
hand
hygiene
in
contact
with
patients;
the
appropriate
practice
of
hand
hygiene
before
and
after
patient
contact
was
increased
significantly
by
65.9%
from
(5.3%
to
46.2%)
pre-post
intervention
while
it
increased
significantly
to
71.2%
of
the
students
after
6
months.
These
results
were
higher
than
other
hand
hygiene
interventions
based
on
observations
where
difference
from
pre
to
post
evaluations
in
overall
hand
hygiene
ranged
from
14%
-27
%
by
other
studies.[16-18]
The
higher
compliance
in
the
present
study
could
be
due
to
the
self
reported
which
is
expected
to
be
much
higher
than
with
direct
observation.
In
another
study
by
KuKanich
et
al.,
Gel
sanitizer
and
informational
posters
were
introduced
together
as
an
intervention
and
they
found
that
hand
hygiene
improved
from
baseline
to
the
intervention
period
for
precontact
and
postcontact
observations,
and
this
improvement
was
sustained
with
no
significant
decreases
in
hygiene
during
the
follow-up
period.
[19]
Although
Self-reported
data
were
not
considered
a
valid
measure
of
compliance
Gould
et
al.,
2010,
[20]
In
a
previous
study,
self
reported
adherence
was
higher
61%
than
observed
practice
44%.[21]
The
current
study
revealed
that
52.3%
didn't
practice
hand
hygiene
with
no
one
practiced
it
before
contact
wit
patient
while
only
1.5%
before
and
after
in
the
pre
intervention.
These
results
were
in
congruent
with
that
found
by
Anwar
et
al.,
[22]
where
only
4.7%
of
the
physicians
reported
to
decontaminate
their
hands
before
direct
contact
with
patients
and
20.9%
after
contact..
The
current
reported
compliance
at
the
start
of
the
study
could
be
related
to
the
lack
of
formal
training
of
most
of
the
students.
Appropriate
time
of
hand
rubbing
as
recommended
by
WHO,
was
observed
among
5.3%
of
the
student
in
the
pre
intervention
that
significantly
was
increased
to
50.8%
in
the
post
intervention
observations
but
it
was
further
increased
among
69.7%
of
the
students
after
6
months-follow
up.
The
higher
compliance
in
the
follow
up
could
explain
the
improvement
in
the
technique
of
hand
hygiene
among
the
students
in
their
second
educational
year.
The
most
inappropriate
hand
washing
at
the
pre
intervention
were
appropriate
time
5.3%;
the
top
and
back
of
fingers
16.7%
and
closing
the
tap
20.5%.
Also
in
a
descriptive
study
by
Abd
Elaziz
and
Bakr[3]
2009,
the
most
common
form
of
inappropriate
hand
washing
was
in
the
improper
drying
and
having
short
contact
time
23.2%.
The
current
study
revealed
high
statistically
significant
pre-post
changes
in
knowledge,
attitude
and
practice
with
previous
training
and
the
greater
differences
were
observed
among
those
who
didn't
receive
training.
Fear
or
a
wish
to
protect
oneself
is
also
a
motivational
factor
in
taking
measures
to
prevent
and
control
of
health
acquired
infections.
Many
medical
students
and
others
learn
by
example
and
in
particular
through
the
influence
of
mentors
or
those
senior
personnel
whom
the
student
admires.
[8]
Statistically
significant
correlations
were
found
between
knowledge,
attitude
and
practice
median
scores
in
all
periods
of
the
study.
With
high
intensity
between
knowledge
and
attitude
relatively
high
intensity
of
correlation
between
knowledge
and
practice
mainly
pre
and
due
to
the
intervention.
The
study
was
not
controlled
trial.
The
researchers
aimed
to
provide
structured
educational
training
to
all
first
year
medical
students,
to
be
continued
rather
than
only
to
involve
the
students
in
a
research.
Compliance
was
assessed
based
on
self-report
for
time
constrains.
Most
of
the
published
researches
that
studied
hand
hygiene
among
medical
students
were
descriptive
that
calls
for
comparison
with
other
intervention
studies
that
included
other
health
care
personnel.
The
intervention
on
hand
hygiene
to
the
first
year
medical
students
was
effective
in
improvement
of
knowledge,
attitude,
practice
and
overall
KAP
of
the
students
after
education
with
further
improvement
after
6
month
in
the
follow
up
in
their
second
educational
year.
Inclusion
and
implementation
of
the
educational
training
on
hand
hygiene
is
recommended
to
the
medical
students
in
health
care
settings.
Acknowledgement:
The
authors
would
like
to
acknowledge
the
participants,
the
tutors
of
the
students,
managers
of
the
primary
care
centers
and
their
health
team
for
facilitation
and
supporting
the
study.
1.
WHO
guidelines
on
hand
hygiene
in
health
care
2009.
Available
from
http://www.who.int/gpsc/5may/tools/9789241597906/en/
[Last
accessed
on
2014
Feb1].
2.
Al
Kadi
A,
Salati
SA.
Hand
Hygiene
Practices
among
Medical
Students.
Interdisciplinary
Perspectives
on
Infectious
Diseases
2012;16:1-6
3.
Abd
Elaziz,
Bakr
IM.
Assessment
of
knowledge,
attitude
and
practice
of
hand
washing
among
health
care
workers
in
Ain
Shams
University
hospitals
in
Cairo.
J
PREV
MED
HYG
2009;50:19-25
4.
van
De
Mortel
TF,
Kermode
S,
Progano
T,
Sansoni
J.
A
comparison
of
the
hand
hygiene
knowledge,
beliefs
and
practices
of
Italian
nursing
and
medical
students.
Journal
of
Advanced
Nursing
2012,
68:569-79
5.
Sansoni
J,
Mariani
P,
De
Caro
W
et
al.,.
Hand
washing:
comparison
between
professionals
and
students
behaviours
in
a
large
University
hospital
of
Rome.
Prof
Inferm.
2011;64:196-206.
6.
Mehtar
S,
Marais
F,
Aucamp
M.
From
Policy
to
Practice
-
Education
in
Infection
Prevention
and
Control.
Int
J
Infect
Control
2011;7:2
7.
Kaur
R,
Razee
H,
Seale
H.
Teaching
the
concepts
of
hand
hygiene
to
undergraduate
medical
students:
the
views
of
key
stakeholders.
Antimicrob
Resist
Infect
Control.
2013;2:143.
8.
Humphreys
H,
Richards
J.
Undergraduate
and
postgraduate
medical
education
on
the
prevention
and
control
of
healthcare-associated
infection.
More
progress
is
needed.
Int
J
Infect
Control
2011;7:1
-
5.
9.
Nair
SS,
Hanumantappa
R,
Hiremath
S
G,
Siraj
MA,2
and
Raghunath
P.
Knowledge,
Attitude,
and
Practice
of
Hand
Hygiene
among
Medical
and
Nursing
Students
at
a
Tertiary
Health
Care
Centre
in
Raichur,
India
ISRN
Preventive
Med
2014;
2014:
608927.
10.
Shinde
MB,
Mohite
VR.
A
study
to
assess
knowledge,
attitude
and
practices
of
five
moments
of
hand
hygiene
among
nursing
staff
and
students
at
a
tertiary
care
hospital
at
Karad
http://www.ijsr.net/archive/v3i2/MDIwMTM5NTc%3D.pdf
[Last
accessed
on
2014
Dec15].
11.
Ariyaratne
MH,
Gunasekara
TD,
Weerasekara
MM,
Kottahachchi
J,
Kudavidanage
BP,
Fernando
SS.
Knowledge,
attitudes
and
practices
of
hand
hygiene
among
final
year
medical
and
nursing
students
at
the
University
of
Sri
Jayewardenepura
Sri
Lankan
Journal
of
Infectious
Diseases
2013
Vol.3(1);15-25.
12.
The
Joint
Commission.
Measuring
Hand
Hygiene
Adherence:
Overcoming
the
Challenges.
Available
from
http://www.jointcommission.org/assets/1/18/hh_monograph.pdf
[Last
accessed
on
2014
Feb
3
].
13.
Huang
J,
Jiang
D,
Wang
X,
et
al.,
Changing
knowledge,
behavior,
and
practice
related
to
universal
precautions
among
hospital
nurses
in
China.
J
Contin
Educ
Nurs
2002;33:217-24.
14.
Rezaee
R,
Danaei
M,
Askarian
M.
The
Efficacy
of
Teaching
hand
Hygiene
to
Medical
students:
An
Interventional
Study.
International
Journal
of
Academic
Research
in
Business
and
Social
Sciences
2014;
4:151-9
http://hrmars.com/index.php/journals/papers/IJARBSS/v4-i9/1138
[Last
accessed
on
2014
Dec1].
15.
Gould
D,
Chamberlain
A.
The
use
of
a
ward-based
educational
teaching
package
to
enhance
nurses'
compliance
with
infection
control
procedures.
J
Clin
Nurs
1997
Jan;6(1):55-67.
16.
Helder
OK,
Brug
J,
Looman
CW,
van
Goudoever
JB,
Kornelisse
RF.
The
impact
of
an
education
program
on
hand
hygiene
compliance
and
nosocomial
infection
incidence
in
an
urban
neonatal
intensive
care
unit:
an
intervention
study
with
before
and
after
comparison.
Int
J
Nurs
Stud
2010
;47:1245-52.
17.
McLaws
ML,
Pantle
AC,
Fitzpatrick
KR,
Hughes
CF.
Improvements
in
hand
hygiene
across
New
South
Wales
public
hospitals:
clean
hands
save
lives,
part
III.
Med
J
Aust
2009;191:S18-24.
18.
Wong
T-W,
Tam
WW-S.
Handwashing
practice
and
the
use
of
personal
protective
equipment
among
medical
students
after
the
SARS
epidemic
in
Hong
Kong.
Am
J
Infect
Control
2005;33:
580-586.
19.
Kukanich
KS,
Kaur
R,
Freeman
LC,
Powell
DA.
Evaluation
of
a
hand
hygiene
campaign
in
outpatient
health
care
clinics.
Am
J
Nurs.
2013;113:36-42
20.
Gould
DJ,
Moralejo
D,
Drey
N,
Chudleigh
JH.
Interventions
to
improve
hand
hygiene
compliance
in
patient
care.
Cochrane
Database
Syst
Rev.
2010;(9):CD005186.
21.
Pittet
D,
Simon
A,
Hugonnet
S,
Pessoa-Silva
CL,
Sauvan
V,
Perneger
TV.
Hand
hygiene
among
physicians:
performance,
beliefs,
and
perceptions.
Ann
Intern
Med
2004;141:1-8.
22.
Anwar
MA,
Rabbi
S,
Masroor
M,
Majeed
F,
Andrades
M,
Baqi
S.
Self-reported
practices
of
hand
hygiene
among
the
trainees
of
a
teaching
hospital
in
a
resource
limited
country.
J
Pak
Med
Assoc
2009;59:631-4.
|
|
.................................................................................................................

|
| |
|
