The
effect of nutritional educational intervention
to mothers on improving the hemoglobin level of
their nine month old children attending Ahmed
Ali Kanoo Health Center in the Kingdom of Bahrain
Fatima
Al Alawi (1)
Watheq A. Hashim (2)
Ghaida Abdulla (1)
Adel Al Sayyad (3)
(1)
Consultant Family Physician, MOH, Kingdom of
Bahrain
(2) Family Physician, MOH, Kingdom of Bahrain
(3) Consultant Family Medicine & Epidemiology,
MOH, Kingdom of Bahrain
Correspondence:
Dr. Fatima Al Alawi,
Consultant
Family Physician, MOH,
Kingdom of Bahrain
Mobile: +973 39454191
Email: dr.falalalwi@gmail.com
|
Abstract
Background:
Anemia is a public health problem
that affects the population of both rich
and poor countries. The WHO's Global Database
considers the prevalence of anemia in
Bahrain as moderate, ranging between 20%-39.9%
in all age groups (5). On the other hand,
the prevalence of anemia is reaching 48.3%
in those who are 6-59 months of age.
Diverse methods of intervention have been
designed to prevent and correct iron deficiency
anemia including the following:
1. Education,
2. Dietary improvement,
3. Fortification of foods with iron,
4. Iron supplementation and,
5. Other public health measures, such
as helminthic control.
The
aim of this study is to observe the effect
of maternal nutritional educational intervention
on correcting iron deficiency anemia of
their children who presented at the health
center for the nine month screening program.
Methodology:
• Mothers and their children at 9
months of age who attended Ahmed Ali Kanoo
health center MCH department for regular
screening from August 2010 until July
2011 were included in the study.
• Booklets were checked for Hb level
at 9 months and later at 18 months, gender,
duration of pregnancy, and hemoglobinopathies
of the children. Moreover, mother's age,
educational level and occupation were
also recorded.
• Mothers of anemic children were
contacted by telephone and asked whether
they received any of the nutritional educational
intervention, and whether they gave their
children the iron supplement or not.
Results:
• The total number of children included
in the study was 448. The Total number
of females was 211 (47.1%) and males 237
(52.9%). The majority of the babies were
delivered full term 426 (95.1%), while
22 (4.9%) were premature.
• The percentage of anemia in infants
at the age of nine months was 198 (45.7%)
while at the age of 18 months it decreased
to 136 (31.9%).
• Seventy-five (19.3%) who had a
low Hb level at 9 months of age improved
to a normal Hb level at 18 months of age.
However, 44 (11.3%) of the infants who
were anemic at 9 months of age continued
to be anemic at 18 months of age.
• Change in Hb level from 9 months
to 18 months of age is not statistically
significant in relation to:
o gender (P=0.086),
o mode of delivery ( P=0.142 ),
o mother occupation (p=0.58),
o mother education (p= 0.468),
o mother age (p=0.141),
o presence of alpha thalassemia (0.264),
o SCD (p=0.375) and,
o whether iron supplementation was given
to child (p= 0.15)
The study showed that nutritional educational
intervention that includes educating the
mother (by doctors, nurses and/or educational
material) was statistically significant
(p= 0.025) in improving anemia from 9
to 18 months of age.
Conclusion:
This study showed a statistically
significant relationship between providing
nutritional educational intervention and
improving the iron deficiency anemia outcome
in nine months old children.
Key words: nutritional, educational,
intervention, anemia, children, Bahrain.
|
Iron status in the human body can be grouped
into normal level, iron depletion, iron deficiency
without anemia and iron deficiency with anemia.
Iron depletion refers to the earliest stage
of diminishing iron stores in the setting of
insufficient iron supply as a result of insufficient
intake or excessive loss of iron. Iron deficiency
(without anemia) develops as these iron stores
are depleted further and begin to impair hemoglobin
synthesis. Finally iron deficiency anemia results
when the supply is insufficient to maintain
normal levels of hemoglobin and represents the
latest spectrum of iron deficiency. (1, 2)
The World Health Organization defines Iron deficiency
Anemia (IDA) as a hemoglobin (Hb) concentration
of 2 SDs below the mean Hb concentration for
a normal population of the same gender, age
range and altitude (2, 3). In the age group
between 6-59 months, anemia is considered to
be present when the hemoglobin level is below
11 g/dl. (4)
Anemia is a public health problem that affects
the population of both rich and poor countries.
The WHO Global Database considers the prevalence
of anemia in Bahrain as moderate, ranging between
20%-39.9% in all age groups (5). On the other
hand, the prevalence of anemia is reaching 48.3%
in those who are 6-59 months of age. (6)
In Saudi Arabia the prevalence of anemia in
the same age group (preschool) ranges between
20%-67% (7). A study done in Riyadh showed that
37.2% of healthy Saudi infants between 6-24
months of age who were attending the Well Baby
Clinic at King Khalid University were found
to be anemic, while the prevalence of anemia
in Jeddah on children of the same age group
was 37.7%. (8) In Western Saudi Arabia, 34%
of the Bedouin children below five years of
age were found to be anemic. (8)
In 2003 the Palestinian Central Bureau of statistics
reported that 37.9% of children aged 6-59 months
were anemic.(9) In a study done in Southwest
Iran for children aged 6-59 months, anemia was
found in 43.9% of children and 29.1% were due
to iron deficiency anemia. The study also shows
that the highest prevalence of iron deficiency
anemia was in the 12-24 months age group.(10)
When it comes to Eastern Mediterranean Region,
Yemen has the highest prevalence of anemia in
preschool age group where the prevalence is
about 73.5%, followed by Pakistan with 60% and
Palestine with 52% prevalence of anemia. (6)
Globally, Africa has the highest prevalence
of anemia in preschool age children with 67.6%,
followed by South East Asia 65.5%, Eastern Mediterranean
46.7%, America 29.3% and Western Pacific 23.1%.
(5)
The least prevalence of anemia was found in
Europe with a prevalence of 21.7 % in preschool
children. (5)
Diverse methods of interventions exist that
are designed to prevent and correct iron deficiency
anemia. These include education, dietary improvement,
fortification of foods with iron, iron supplementation,
and other public health measures, such as helminthic
control (11).
Many studies have been conducted showing the
various effects of education on preventing and
treating iron deficiency anemia.(12-15) A pilot
study in Tehran in 2001 showed an increase in
ferritin levels in those children whose mothers
received nutrition education as compared to
the control and dietary modification groups.(12)
A randomized trial conducted in Delhi, India
in 2003 suggested that nutrition education did
have a positive effect on the iron status possibly
by improving the dietary iron intake.(13) Another
study in UAE in 2005 showed highly significant
increases in the levels of hemoglobin and hematocrit
of children of mothers who received a face to
face health education program.(14) A recent
study in 2013 in Iran showed that education
based on health belief model can improve knowledge
of parents towards supplemental iron. (15)
On the other hand, a Randomized Clinical Trial
(RCT) in west and south Birmingham, in 1997
showed no reduction in anemia using a targeted
nutritional program and have highlighted the
difficulties in conducting health education
programs within the scope of current health
resources. (16) In 2012 a study in Brazil, on
maternal dietary counseling covering breastfeeding
and healthy complementary feeding on the prevalence
of iron deficiency, anemia and iron deficiency
anemia in children aged 12 to 16 months showed
no effect of dietary counseling on the prevalence
of anemia, iron deficiency or iron deficiency
anemia.(17)
The aim of this study is to observe the effect
of maternal education on correcting iron deficiency
anemia.
In the Kingdom of Bahrain, the primary health
care services are provided through 25 health centers
distributed all over the kingdom.(18) Ahmed Ali
Kanoo health center is one of those health centers
that provide primary health services to a population
of around 35,000. Maternal and child health department
(MCH) in the health center is providing all the
health care services to mothers and children.(18)
Child screening is one of the major services provided
that include anemia screening at 9 months of age.
Mothers and their children at 9 months of age
who attended the MCH department in Ahmed Ali
Kanoo Health Center for regular screening program
in the period from August 2010 to July 2011
were included in the study.
According to the MCH guidelines, mothers and
care givers of children with low Hb (below 11
at 9 months) are supposed to receive nutritional
educational intervention including advice from
nurses, doctors and/or receiving educational
leaflets regarding diet and iron supplementation.
(19) They should also be given iron supplementation
according to the weight of the child. Booklets
were checked for Hb level at 9 and later at
18 months, gender, duration of pregnancy, and
heamoglobinopathies of the children. Moreover,
mother age, educational level and occupation
were recorded.
Mothers of anemic children were contacted then
by telephone and asked whether they received
any of the nutritional educational intervention,
and whether they gave their children the iron
supplement or not. Data were entered in excel
and transferred to SPSS. Continuous variables
were presented as means and standard deviation
and categorical variables were presented as
percentages. Chi square test was used for association
testing.
• The total number of children included
in the study was 448. (Table 1)
• The total number of females was 211 (47.1%)
and the males were 237 (52.9%).
• Most of the babies were delivered full
term 426 (95.1%), and only 22 (4.9%) were premature.
(Table 1)
• Our sample showed a total of 95 (21.1%)
infants carry the alpha thalassemia gene, 8
(1.8%) had sickle cell disease, and 2 (0.4%)
had beta thalassemia trait. (Table 1)
• Most of the mothers were housewives 304
(68.2%), and only 142 (31.8%) were working.
(Table 1)
• Around half of the mothers 226 (50.8%)
had a higher education level, 171 (38.4%) had
a secondary level, and only 48 (10.8%) had an
intermediate level and below. (Table 1)
• The majority of mothers were aged between
30-39 years with a total number of 243 (54.2%);
those who were 30 years and below represent
153 (34.2%), and those who were above 40 years
of age represent 52 (11.6%). (Table 1)
• Most of the infants 121 (92.4%) were
not given iron supplemental therapy by their
mothers, while only 10 (7.6%) were given iron
therapy for a duration of one month and more.
(Table 2)
• For a hundred and twenty-five (80.1 %)
of those who were anemic, their mothers received
the nutritional educational intervention, while
31 (19.9 %) mothers denied receiving any kind
of intervention. (Table 2)
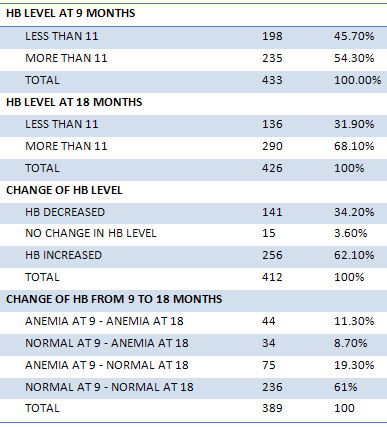
• The percentage of anemia in infants at
the age of nine months was 198 (45.7%) while
at the age of 18 month it decreased to 136 (
31.9%). (Table 3)
• Regardless of being anemic or not, a
total of 256 (62.1%) infants had an increase
in their Hb level from nine to 18 months of
age, while141 ( 34.2%) had a decrease in their
Hb level, and only 15 (3.6%) had the same Hb
level. (Table 3)
• Most of the infants who had a normal
Hb level at 9 months of age continued to have
a normal Hb level at 18 months of age with a
total number of 236 (61%). However, 34 (8.7%)
who had a normal Hb level at 9 months of age
had a drop in their Hb level at 18 months of
age. (Table 3)
• Seventy-five (19.3%) who had a low Hb
level at 9 months of age improved to a normal
Hb level at 18 months of age. However, 44 (11.3%)
of the infants who were anemic at 9 months of
age continued to be anemic at 18 months of age.
(Table 3)
• Change in Hb level from 9 months to 18
months of age is not statistically significant
in relation to gender (P=0.086), mode of delivery
(P=0.142), mother occupation (p=0.58), mother
education (p=0.468), mother age (p=0.141). (Table
4)
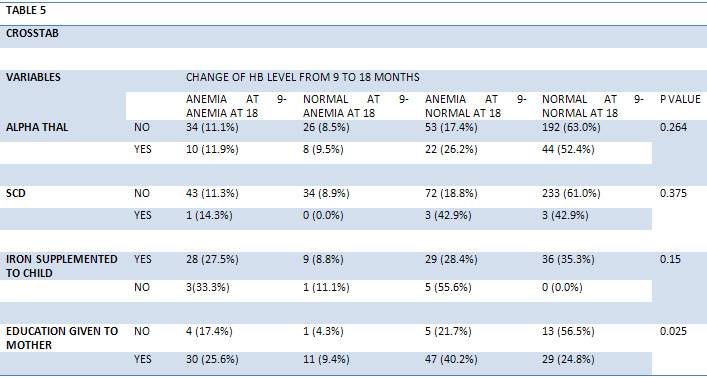
• The presence of alpha thalassemia was
(0.264), SCD (P=0.375), and whether iron therapy
was given to child (P= 0.15) was not statistically
significant in relation to improving the Hb
level from 9 to 18 months of age. (Table 5)
• The study showed that nutritional educational
intervention was statistically significant (P=
0.025) in improving anemia from 9 to 18 months
of age. (Table 5)
Table 1: Characteristics of children at 9
months of age and their mothers who attended
Ahmed Ali Kanoo health centers during August
2010 to July 2011
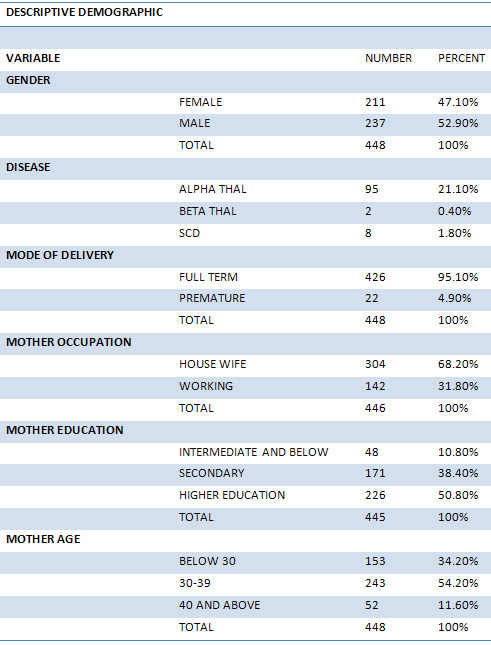
Table 2: Clinical description of Iron supplementation
and nutritional educational intervention to
mothers of anemic 9 month old children who attended
Ahmed Ali Kanoo health center during August
2010 to July 2011
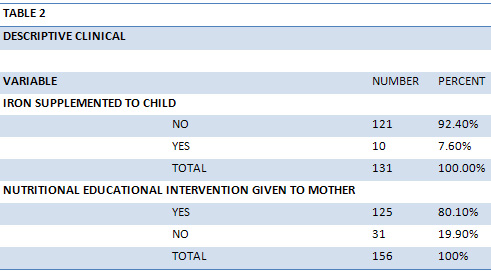
Table 3: Hb Status of children at 9 and
18 months who attended Ahmed Ali Kanoo health
centers during August 2010 to July 2011
Click here for Table
4: Effect of demographic variables on the Hb
status of children at 9 and 18 months who attended
Ahmed Ali Kanoo health centers during August
2010 to July 2011
Click here for
Table 5: Effect of diseases, iron supplement
and nutritional educational intervention on
the Hb status of children at 9 and 18 months
who attended Ahmed Ali Kanoo health centers
during August 2010 to July 2011
The study showed the percentage of anemia in infants
aged 9 months was 45.7%, which is in concordance
with The WHO Global Database that estimated the
prevalence of anemia in Bahrain to be 48.3% in
those who are 6-59 months of age.(5)
In 2007, a Ministry of Health report showed that
26% of individuals attending for the premarital
counseling service had an alpha thalassemia gene,
and our study also showed that there is a high
percentage of alpha thalassemia reaching 21.1%
in 9 month old infants.(20)
A neonatal screening study done in Bahrain in
1984-1985 showed that the prevalence of sickle
cell disease was 2.1% and decreased to 0.9% in
another study done in 2002(20). In our study,
the percentage of sickle cell disease was high
reaching 1.8 %. This could be due to the high
rate of sickle cell disease in the area of the
study population.
Presence of alpha thalassemia gene and sickle
cell disease were not related to the improvement
of Hb level between 9 and 18 months of age as
expected in these diseases. (21-23)
There were a small percentage of mothers who used
the iron supplement for more than one month to
treat anemia in their infants. This is largely
due to the fact that mothers are worried about
the side effect of iron syrup, such as dental
discoloration, dental carries and constipation.
(24, 25) Moreover it has an un-pleasant taste.
Our study showed that the nutritional educational
intervention of the mother had a statistically
significant role in improving the Hb level in
children between 9 and 18 months of age. This
result is supported by many other studies done
in different regions like UAE, India and Iran
which showed that maternal education significantly
increases the level of hemoglobin in their children(12-14).
Based on the results of the study, we recommended
strengthening the nutritional educational intervention
provided by doctors, nurses and/or other health
professionals in order to improve the uptake of
iron and decrease the prevalence iron deficiency
anemia among children in Bahrain.
This study showed a statistically significant
relationship between providing nutritional educational
intervention and improving iron deficiency anemia.
1)
Chew
E,
Lam
J.
Diagnosis
and
Management
of
Iron
Deficiency
Anaemia
in
Children-
A
clinical
Update.
Proceeding
of
Singapore
Healthcare
2012;21(4):278-285.
http://www.singhealthacademy.edu.sg/Documents/
Publications/Vol21No42012/10%20RA_%20035-0812%20%20Elaine%20Chew.pdf
(accessed
29
December
2013).
2)
University
of
Chicago,
Department
of
Pediatric.
Iron
Deficiency.http://pediatrics.uchicago.edu/chiefs/ClinicCurriculum/documents/IRONDEFICIENCY.pdf
(accessed
29
December
2013).
3)
Baker
R,
Greer
F.
Diagnosis
and
Prevention
of
Iron
Deficiency
and
Iron-Deficiency
Anemia
in
Infants
and
young
Children
(0-3
Years
of
Age).Official
Journal
of
the
American
Academy
of
Pediatrics
2010;126:1040.doi:10.1542/peds.2010-2576.
(accessed
29
December
2013).
4)
Patient.co.uk.
Childhood
Anemia.
http://www.patient.co.uk/doctor/childhood-anaemia.
(accessed
29
December
2013).
5)
World
Health
Organization.
Worldwide
Prevalence
of
Anemia
1993-2005,
WHO
Global
Database
on
Anemia.
http://apps.who.int/iris/bitstream/10665/43894/1/9789241596657_eng.pdf.
(accessed
28
December
2013).
6)
Bagchi
K.
Iron
Deficiency
Anaemia-
An
Old
Enemy.
La
Revue
de
Santé
de
la
Méditerranée
orientale
2004;10(6)754-760.
http://applications.emro.who.int/emhj/1006/10_6_2004_754_760.pdf.
(accessed
10
December
2013).
7)
Musaiger
AO.Iron
Deficiency
Anaemia
in
the
Arab
Gulf
Countries:
The
Need
for
Action.
Bahrain
Medical
Bulletin
2001;23(3)
http://www.bahrainmedicalbulletin.com/june_2001/Editorial.pdf.
(accessed
1
December
2013).
8)
Madani
KA,
Kumosani
T.
Micronutrients
Status
in
Saudi
Arabia.
Bahrain
Medical
Bulletin
2001;23(3):135-39.
http://www.bahrainmedicalbulletin.com/September_2001/Micronutrient.pdf.
(accessed
8
December
2013).
9)
Alhani
HM.
Micronutrient
Deficiency
in
the
Middle
East.
Modern
Medicine2011;28:7.http://www.nestlenutrition-institute.org/country/ae/resources/Library/Free/conferenceproceedings/Conference4/
Documents/DR.%20HATEM%20M.%20ALHANI.pdf.
(accessed
21
December).
10)
Bijan
K
et
al.
Iron
deficiency
anemia
among
children
in
southwest
Iran.
Food
&
Nutrition
Bulletin
2007;28(4):406-411.
http://www.ingentaconnect.com/content/nsinf/fnb/2007/00000028/00000004/art00005.
(accessed
21
December
2013).
11)
WHO.Int.Guidelines
for
the
Use
of
Iron
Supplements
to
Prevent
and
Treat
Iron
Deficiency
Anemia.
http://www.who.int/nutrition/publications/micronutrients/guidelines_for_Iron_supplementation.pdf
(accessed
27
December
2013).
12)
Khoshnevisan
F,
Kimiagar
M,
Kalantaree
N,
Valaee
N,
Shaheedee
N.
Effect
of
Nutrition
Education
and
Diet
Modification
in
Iron
Depleted
Preschool
Children
in
Nurseries
in
Tehran:
a
Pilot
Study.
Int
J
Vitam
Nutr
Res
2004;
74(4):264-68.
http://medcontent.metapress.com/content/b12318326q085128/
(accessed
28
December
2013).
13)
Kapur
D,
Sharma
S,
Agarwal
KN.
Effectiveness
of
Nutrition
Education,
Iron
Supplementation
or
both
on
Iron
Status
in
Children.
Indian
Pediatrics
2003;
40:1131-1144.
http://www.indianpediatrics.net/dec2003/dec-1131-1144.htm
(
accessed
28
December
2013).
14)
Hassan
A,
Kammal
M,
Fetohy
E,
Turkey
G.
Health
education
program
for
mothers
of
children
suffering
from
iron
deficiency
anemia
in
United
Arab
Emirates.
The
Journal
of
the
Egyptian
Public
Health
Association
2005;
80(5-6):525-45.
http://europepmc.org/abstract/MED/17187741/reload=0;jsessionid=sJyKlvQIMyzbPVlGYZIR.24
(accessed
28
December
2013).
15)
Masoome
A,
Marziye
R,
Forough
M.
The
Effects
of
Education
Based
on
Health
Belief
Model
on
Giving
Supplemental
Iron
to
Children
Aged
Between
6
and
24
Months.
International
Electronic
Journal
of
Medicine
2013;
2(2):82-88.
http://www.iejm.net/browse.php?a_id=50&slc_lang=en&sid=1&ftxt=1
(accessed
20
December
2013).
16)
Childs
F,
Aukett
A,
Darbyshire
P,
Ilett
S,
Livera
L.
Dietary
Education
and
Iron
Deficiency
Anemia
in
Inner
City.
Archives
of
Disease
in
Childhood
1997;
76:
144-147.
http://www.ncbi.nlm.nih.gov/pmc/articles/PMC1717082/pdf/
v076p00144.pdf
(accessed
20
December
2013).
17)
Bortolini
G,
Vitolo
M.
The
Impact
of
Systematic
Dietary
Counseling
during
the
First
Year
of
Life
on
Prevalence
Rates
of
Anemia
And
Iron
Deficiency
at
12-16
Months.
Jornal
de
Pediatria
2012;
88(1):
33-39.
http://www.jped.com.br/conteudo/12-88-01-33/port.pdf
(accessed
28
December
2013).
DIO
10.2223/JPED.2156
18)
Kingdom
of
Bahrain,
Ministry
of
Health,
I
seha.
Health
Centers.
http://www.moh.gov.bh/EN/MOHServices/Services/OurPrimaryServices/HealthCenter.aspx
(accessed
27
September
2014).
19)
Kingdom
of
Bahrain,
Ministry
of
Health,
Health
Promotion
Council.
Guidelines
for
Management
of
Child
screening
in
primary
care
setting
and
outpatient
clinics
in
the
Kingdom
of
Bahrain.
http://sites.google.com/site/drwatheq/child%20screening%20Guideline-1.pdf?attredirects=0&d=1
(accessed
27
November
2013).
20)
Al-Arayyed
S,
A
Aziz
H,
Sultan
B,
Shome
D.K,
Bapat
J.P.
Neonatal
Screening
for
Genetic
Blood
Diseases.
Bahrain
Medical
Bulletin
2007;
29(3):
415-9
http://www.bahrainmedicalbulletin.com/September_2007/neonatal_screening.pdf
(accessed
3
January
2014).
21)
Medscape.
Alpha
Thalassemia
Treatment
&
Management
http://emedicine.medscape.com/article/955496-treatment#aw2aab6b6b2.
(accessed
24
September
2014).
22)
The
New
York
Times.
Health
guide:
Thalassemia.
http://www.nytimes.com/health/guides/disease/thalassemia/overview.html
(accessed
on
24
September
2014).
23)
Herbert
L,
Muncie
JR,
James
S,
Campbell.
Alpha
and
Beta
Thalassemia.
Am
Fam
Physician
2009
Aug
15;
80(4):339-344.
http://www.aafp.org/afp/2009/0815/p339.html
(accessed
on
20
August
2014).
24)
WebMD.Find
a
Vitamin
or
Supplement.Iron
http://www.webmd.com/vitamins-supplements/ingredientmono-912-iron.aspx?activeingredientid=912&activeingredientname=iron
(accessed
on
22
September
2014).
25)
Drugs.com.
Iron-150
Side
Effects
http://www.drugs.com/sfx/iron-150-side-effects.html
(accessed
on
22
September
2014).
|


{kind=link}