Health
of Migrant Workers; A Matter Of Concern
Faisal
Abdul Latif Alnasir
Correspondence:
Faisal Abdul Latif Alnasir FPC, MICGP, FRCGP,
FFPH, PhD
Professor of Family Medicine
Chairman; Dept. of Family and Community Medicine
College of Medicine and Medical Sciences
Arabian Gulf University
Former president; Scientific Council for Family
& Community Medicine of the Arab Board for
Health Specialties
Email:
faisal.alnasir@gmail.com
|
Abstract
Over
the past few decades, mobility of people
around the world has been incrementing,
from about 82 million in 1970 to 200 million
in 2005. It customarily transpires to
both developed (which is the majority,
60%) and developing countries for a more
preponderant life opportunity. The most
astronomically immense migrants were found
to settle, in Europe followed by Asia
and North America. In 2000, the European
countries received 56.1 million migrants,
Asia 49.9 million, North America 40.8
million and Africa 16.3 million.
The Middle East, and in particular the
Gulf countries (GCC) have had a tremendous
influx of migrant workers (around 16 million,
the majority, over 80%, were from Asia)
due to its rapid development as reflected
by marked increase in oil revenue. It
is reported that over the past 10 years
almost seven out of every ten members
of the workforce in the GCC were foreigners.
Health issues impacting migrant workers
are intricate and numerous, especially,
when some host countries perceive these
workers as exploitable, frugal and flexible
labor. Despite that most of them work
in 3D jobs; Dirty, Dangerous and Degrading.
They usually have poor living and safety
conditions and the prominent consequential
factor leading to their health disparities
is the cultural differences affecting
their health care seeking patterns, perception
of health and compliance with treatment.
In this review article the health quandaries
of the migrant worker in the GCC countries
and factors playing in worsening those
conditions, are elaborated. Withal we
endeavor to find how to compact such health
issues for the benefit of both the workers
and the nation.
Key words: health,
migrant workers
|
Mobility of people around the world is perpetual
and has never ceased since archaic time. People
kinetically circumnavigate for many reasons,
but economic factors and probing for a more
preponderant life and future shape the most
consequential issues for such acts. It has been
estimated that three percent of the total world
population peregrinates to other countries while
the international mobility over the past four
decades has doubled, incrementing from 82 million
in 1970 to 200 million in 2005 [1].
For migrants who travel abroad for working purposes,
the story is the same. Albeit, their number
has been reported to be perpetually high, during
the last century it has risen sharply due to
rapid worldwide development. About 105 million
people peregrinate abroad to work annually.
Although, such migration occurs in both the
developed and developing worlds, the majority
(around 60%) settle in the developed countries.
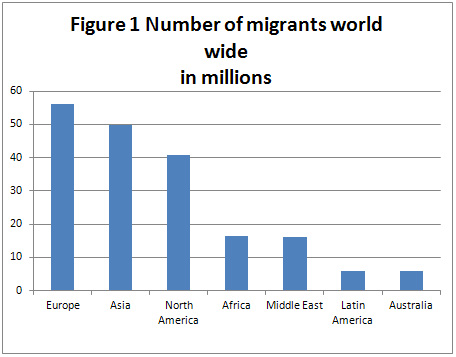
It was reported that the most immensely colossal
single majority of migrants has settled in Europe,
followed by Asia and North America. In 2000,
Europe received 56.1 million migrants, Asia
49.9 million, North America 40.8 million, Africa
16.3 million, Middle East 16.00 million, Latin
America 5.9 million and Australia 5.8 million
migrants[1], (Figure 1). However, The United
States is still considered to be the most attractive
place for many migrants around the world.
Migration is not constrained to certain sectors
or nationalities but it occurs from virtually
all countries, in particular poor nations. According
to the Philippines Overseas Employment Administration
(POEA) more than ten million Filipinos have
left seeking for jobs because of high unemployment
levels in their country, of whom, the majority
went to the Arab world (around 200,000 in Saudi
Arabia alone)[2]. And the Filipino emigration
towards the Middle East has grown by 29.5 per
cent between 2007 and 2008[2].
In addition migration is not limited to a certain
gender as women today are found to represent
around half of the total international migrants
worldwide. Eighty three percent of all domestic
workers in the world are women. And the percentage
of women's employment in particular in Europe
is increasing as betokened by the third European
survey on working conditions[3].
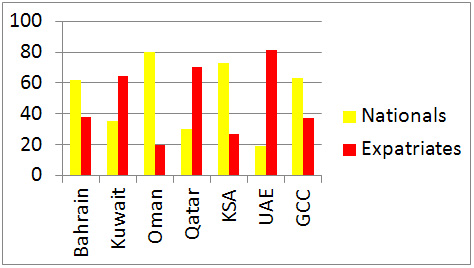
Due to the economic boom during the last fifty
years, the Middle East (ME) in general and the
Gulf Coopration Countries (GCC) in particular,
have attracted many migrant workers from all
around the world. Studies reported that in the
1980s, over 80% of these countries' workers
emanated from Asia (of whom 20% were Indians)
and almost seven out of ten of its workforce
are foreigners[4,5], to the extent that 90%
of all workforce population in Qatar and the
UAE alone, are expatriate[6] (Figure 2).
Andrzej Kapiszewski in his study in 2001 while
illustrating the GCC migrant workers' nationalities
denoted that in almost all of these countries,
Indian formed the majority[7] .
Despite the fact that the contribution of the
immigrant workers to the host country's economy
can't be estimated, it is unfortunate that in
many instances they are perceived as exploitable,
frugal and flexible labor, and therefore employed
in 3-D jobs: Dirty, Dangerous and Degrading[8].
Kawon et al., (2011) reported that these migrants
are often depicted as an encumbrance on society[9].
Hence they face earnest health quandaries due
to discrimination, their licit position, low
socioeconomic status or due to language barrier[10].
Moreover, many of them often face difficulties
in adjusting to their new society including
adopting safe and healthy lifestyles because
the nature and quality of health care and the
gregarious and health characteristics of re-settlement
can withal determine the health status of migrants.
Health issues impacting migrant workers are
intricate and numerous and factors that affect
their health are vast and varied, of which the
cultural difference in attaining health is one
of the most consequential. When tailoring interventions
to vulnerable populations, consideration ought
to be given to the importance of diverse cultural
beliefs. Since culture shapes an individual's
perception of health, illness, and compliance
with diagnosis and treatment regimens. Cultural
differences in health care seeking patterns
and differences in the perception of health
care could markedly affect their health status[11].
In addition, the workers' educational level
plays a vital role in their health status. A
recent study concerning the health and lifestyle
of Nepalese migrants in the United Kingdom has
found that migrants with low level of education
are more likely to lack good dental hygiene
and regular exercise[12].
The precedent medical history of migrants, is
also important since certain diseases are cognate
to their nationalities. A study from the UAE
reported that the obesity rate was high among
certain nationalities while the presence of
hepatitis C antibodies was virtually exclusive
to, more or less, Egyptian workers[13].
Other barriers that put migrant workers in situations
of vulnerability and risk of ill health are
factors that are related to lack of knowledge
of the health system and precarious work or
exposure to higher risk working and occupational
hazards and accidents. Occupational injuries
and work accidents have a contribution on the
health and the well-being of migrant workers.
In highlighting that, the Nepalese government
recently revealed that about 70 of their nationals
died on building sites in one of the GCC countries
since the beginning of 2012. Hundreds more are
thought to have been injured in falls and accidents
with machinery and vehicles[3]. Accommodation
on the other hand forms a major health risk
factor and workers health after migration could
also deteriorate due to the living conditions.
Conventionally workers live in an overcrowded
insalubrious condition that lacks sanitation
and is an environment for deterioration of physical
and mental health. The mental health status
and salubrity is also influenced by life-adjustment
stressors, socioeconomic isolation and cultural
alienation from mainstream society which result
in somatization issues. Workers from poorer
groups are usually at a higher risk of mental
illness due to their living and working conditions.
Women migrant worker are no different, beside
being at risk of acquiring many health hazards
especially physical, they are prone to sexual
and verbal abuse. The International Labor Organization
(ILO) reported that Indonesian women migrant
workers, a majority of whom work as domestic
workers, are particularly vulnerable to gender
predicated violence and to HIV that avails throughout
the employment period[5]. The POEA also indicated
that some Filipino female workers face horrible
working conditions as well[2].
In highlighting the health problem of the migrant
workers, the BSR Migration Linkage's report
in 2012[14] has stipulated four focal stations,
that contribute to the health of any migrant
worker: those which are related to pre-departure
and transit such as the health risk and poor
health in the country of origin and cultural
beliefs that affect health; post-arrival factors
suchas language barrier, employment in 3-D jobs
and lack of access to adequate health care services;
while at work such as the inadequate living
conditions, inadequate nutrition and greater
susceptibility to mental health strains. And
the last factor is related to when workers return
to their county of origin such as lack of awareness
of medium and long-term illnesses that can leave
workers at heightened risk upon return.
To procure equitable, adequate, and efficacious
access to health care services, migrants need
initially to be inculcated and apprised about
the health care system and how to approach it
in the country of work. The more workers become
integrated the more they would utilize health
care services efficaciously[15].
It is the legal obligation of countries of destination,
origin and transit to protect the human rights
of migrants on their territory[3]. Countries
that are dependent on migrant workers should
review their health and safety procedures in
order to prepare a healthy working envoironmet
for such workers. For such causes and in order
to facilitate health accessibility for migrant
workers the ILO in 1997 adopted guidelines "The
Workers' Health Surveillance" that place
workers' health surveillance within the discipline
of occupational safety and health. The central
purport is the primary obviation of occupational
and work-cognate diseases and injuries. These
provisions are considered to be the rudimentary
requisites for the surveillance of workers'
health, and are not intended to deter competent
ascendant entities from adopting higher standards[10].
In that line the GCC countries started the implementation
of proper screening programs for foreign workers
in order to protect their health and to prevent
the entry of possible infection that might be
dangerous to their population. It includes epidemiological,
psychological, neurological and sexual examinations
and investigations besides other tests ensuring
the public safety[16]. Despite that, most of
workers in the GCC countries, are initially
screened at employment, but without a strict
longitudinal follow up.
To ensure the provision of a proper health service
to migrant workers, Poureslami et al, recommended
adopting multiple approaches, that include;
mapping and identifying health risks for major
migrant workers; building health profiles at
the pre-departure phase; ensuring occupational
health and safety procedures are communicated
and enforced effectively to migrant workers;
taking proactive steps to ensure the availability,
accessibility, and acceptability of health services
in the destination country; educating the migrants
about how to approach such facilities; to overcome
the language barriers and finally avoiding overcrowding
in accommodation compounds[17].
In conclusion, health issues impacting migrant
workers are intricate and numerous. Therefore,
their health provision should always be the
responsibility of the government and not delegated
to private sectors in order to ensure proper
adoption and implementation of health policies
for the health safety of these workers and the
nation.
1-
Pratik
Adhikary,
Steven
Keen,
Edwin
van
Teijlingen.
Health
Issues
among
Nepalese
migrant
workers
in
the
Middle
East
Health
Science
Journal.
2011;
5,
3
2-
Digal
Santosh.
Christian
Filipino
migrants
forced
to
convert
to
Islam.
2010
http://www.asianews.it/news-en/Christian-Filipino-migrants
3-
Domestic
workers
across
the
world:
Global
and
regional
statistics
and
the
extent
of
legal
protection.
International
Labour
Office
Geneva.
ILO,
2013
4-
Newson-Smith
MS.
Importing
health
conditions
of
expatriate
workers
into
the
United
Arab
Emirates.
Asia
Pac
J
Public
Health.
2010
Jul;22(3
Suppl):25S-30S.
5-
Andrzej
Kapiszewski.
Arab
versus
Asian
migrant
workers
in
the
GCC
countries.
UN/POP/EGM/2006/02.22
May
2006
6-
Côté
D.
Intercultural
communication
in
health
care:
challenges
and
solutions
in
work
rehabilitation
practices
and
training:
a
comprehensive
review.
Disabil
Rehabil.
2013
Jan;35(2):153-63.
7-
Andrzej
Kapiszewski.
(2001)
Nationals
and
Expatriates:
Population
and
Labour
Dilemmas
of
the
Gulf
Cooperation
Council
States.
Ithaca
Press.
8-
Lindsay
S,
King
G,
Klassen
AF,
Esses
V,
Stachel
M.
Working
with
immigrant
families
raising
a
child
with
a
disability:
challenges
and
recommendations
for
healthcare
and
community
service
providers.
Disabil
Rehabil.
2012;34(23):2007-17.
9-
Lee,
Kawon;
McGuinness,
Connor;
Kawakami,Tsuyoshi.
Research
on
occupational
safety
and
health
for
migrant
workers
in
five
Asia-Pacific
countries:
Australia,
Republic
of
Korea,
Malaysia,
Singapore
and
Thailand/Kawon
Lee,
Connor
McGuinness
and
Tsuyoshi
Kawakami;
ILO
DWT
for
East
and
South-East
Asia
and
the
Pacific.
-
Bangkok:
ILO,
2011
10-
Technical
and
ethical
guidelines
for
workers'
health
surveillance
(OSH
No.
72).
Geneva,
International
Labour
Office,
1998
(Occupational
Safety
and
Health
Series
No.
72)
11-
National
Institute
of
Health.
Addressing
health
disparities:
The
NIH
program
of
action
2002.http://www.healthdisparities.nih.gov/whatare.html
12-
Adhikary
P,
Simkhada
P,
van
Teijlingen
E.
Raja
A.
Health
and
lifestyle
of
Nepalese
migrants
in
UK.
BMC
Int
Health
Human
Right.2008;
8:6
Available
at:
http://www.biomed
central.com/1472-698X/8/6
Accessed
on
03/03/2010
13-
Newson-Smith
MS.Importing
health
conditions
of
expatriate
workers
into
the
United
Arab
Emirates.Asia
Pac
J
Public
Health.
2010
Jul;22(3
Suppl):25S-30S
14-
Migrant
workers
and
health-
the
role
of
business.
BSR
-Migration
Linkages
January
16,
2012;
http://www.bsr.org/reports/BSR_Migration_Linkages_Migration_and_Health.pdf
15-
Dastjerdi
M.The
case
of
Iranian
immigrants
in
the
greater
Toronto
area:
a
qualitative
study.Int
J
Equity
Health.
2012
Feb
27;11:9.
16-
Gulf
controls
to
prevent
the
entry
ailing
labor
(Arabic)
http://www.alraimedia.com/alrai/Article.aspx?id=474801&date=0311201313
17-
Poureslami
I,
Rootman
I,
Doyle-Waters
MM,
Nimmon
L,
Fitzgerald
JM.
Health
literacy,
language,
and
ethnicity-related
factors
in
newcomer
asthma
patients
to
Canada:
a
qualitative
study.
J
Immigr
Minor
Health.
2011
Apr;13(2):315-22.
|

