|
|
 |
| ............................................................. |
|
|
| ........................................................ |
| From
the Editor |

|
Editorial
A. Abyad (Chief Editor) |
|
|
|
|
........................................................
|
Original
Contribution/Clinical Investigation
|
|
|
<-- Turkey / International -->
Enuresis
Nocturna and the Symptoms of Upper Airway Obstruction
in Primary School age Children: Is there a Relationship?
[pdf
version]
Doganer Yusuf Cetin, Aydogan Umit , Ashfaq Tabinda,Burmaoglu
Serhat, Sari Oktay Koc Bayram, Saglam Kenan,
Qidwai Waris
<-- Sri Lanka -->
Referral
communications: Bridging the gap between primary
care doctors and specialists
[pdf
version]
R.P.J.C. Ramanayake, A.H.W. de Silva, D.P. Perera,
R.D.N. Sumanasekera, K.M.S.
Lakmini, B.L.S. Ranasigh
Appendix:
Click here for a template Referral form
<-- Jordan -->
Sodium
Stibogluconate treatment for cutaneous leishmaniasis:
A clinical study of 43 cases from the north
of Jordan
[pdf
version]
Mamoun Mohammad Al-Athamneh, Hiathem Qasem Abu
Al-haija, Ra’ed Smadi, Ayman S. Qaqaa ,Heba
Ajlouni
|
|
........................................................ |
Medicine and Society
........................................................
Clinical Research and
Methods
.......................................................
Continuing
Medical Education
|
Chief
Editor -
Abdulrazak
Abyad
MD, MPH, MBA, AGSF, AFCHSE
.........................................................
Editorial
Office -
Abyad Medical Center & Middle East Longevity
Institute
Azmi Street, Abdo Center,
PO BOX 618
Tripoli, Lebanon
Phone: (961) 6-443684
Fax: (961) 6-443685
Email:
aabyad@cyberia.net.lb
.........................................................
Publisher
-
Lesley
Pocock
medi+WORLD International
11 Colston Avenue,
Sherbrooke 3789
AUSTRALIA
Phone: +61 (3) 9005 9847
Fax: +61 (3) 9012 5857
Email:
lesleypocock@mediworld.com.au
.........................................................
Editorial
Enquiries -
abyad@cyberia.net.lb
.........................................................
Advertising
Enquiries -
lesleypocock@mediworld.com.au
.........................................................
While all
efforts have been made to ensure the accuracy
of the information in this journal, opinions
expressed are those of the authors and do not
necessarily reflect the views of The Publishers,
Editor or the Editorial Board. The publishers,
Editor and Editorial Board cannot be held responsible
for errors or any consequences arising from
the use of information contained in this journal;
or the views and opinions expressed. Publication
of any advertisements does not constitute any
endorsement by the Publishers and Editors of
the product advertised.
The contents
of this journal are copyright. Apart from any
fair dealing for purposes of private study,
research, criticism or review, as permitted
under the Australian Copyright Act, no part
of this program may be reproduced without the
permission of the publisher.
|
|
|
| September 2014
- Volume 12 Issue 7 |
|
Scabies
in children in sector Gaza
Thaer
Almomani
Correspondence:
Thaer Almomani MD, JBP
Department of Pediatrics, Royal Medical Services.
Irbid, Jordan
Tel: ++962 0777260153
Email:
thaer_mom@yahoo.com
|
Abstract
Objectives: To
present a profile of scabies in children
in sector Gaza.
Methods: All
patients who were seen in the outpatient
clinic in Jordanian hospital in Gaza between
25/11/2010 and 24/01/2011 and who presented
with itching, were examined for scabies.
Patients were divided into three age groups:
group I: 0-4 years, group II: 4-8 years
and group III: 8-14 years.
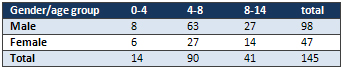
Results: A
total of 5430 children were seen in outpatient
clinic for various diseases and conditions
during the study period. 145 cases of
scabies were reported with 98 males and
47 females. Scabies was higher in age
group II: age 4-8 years, followed by group
III; 8-14 years. The incidence of scabies
among children seen in the clinic was
0.02% and was higher in males. The commonest
manifestation was night itching followed
by skin marks.
Conclusion: Scabies
is a common disease among children in
Gaza. Major contributing factors to this
disease are: crowding, poor hygiene, scarce
water supplies and low socio-economic
class.
Key words: scabies,
children, Gaza
|
Scabies is an infectious skin disease caused by
S. scabiei var. hominis. According to the WHO
about 300 million persons per year develop scabies
worldwide.(1) Scabies is a common dermatological
problem managed by both pediatricians and dermatologists.
It manifests itself in various forms in children
and differs from that in adults in many ways.
The primary contributing factors in contracting
scabies seem to be poverty and overcrowded living
conditions. The incidence rate of scabies is 28/100,000
inhabitants. The incidence is higher in the elderly
(51/100, 000 in persons aged >75 years) and
a higher incidence was also found in immigrants
(88/100,000).(2)
Scabies is highly contagious and is spread from
person to person by direct skin contact. Transfer
from clothes and bedding occurs rarely and only
if contaminated by infectious people immediately
beforehand.(3) Infestation occurs when pregnant
female mites burrow into the skin and lay eggs.
After two or three days the larvae emerge and
dig new burrows. They mature, mate, and repeat
this cycle every two weeks. The main symptoms
of scabies are caused by the host immune reaction
to burrowed mites and their products.(4) Symptoms
appear within two to six weeks of the initial
infestation, but reinfestation can provoke symptoms
within 48 hours.
The most common presenting lesions are papules,
vesicles, pustules, and nodules. The pathognomonic
sign is the burrow-a short, wavy, grey line that
is often missed if the skin is eczematised, excoriated,
or impetiginised. (5)
The purpose of this study is to present data on
scabies in children seen at the Jordanian field
hospital in Gaza strip.
All children attending the pediatric outpatient
clinic at the Jordanian field hospital in Gaza
between 25/11/2010 and 24/01/2011,with itching,
were included in this prospective study. Patients
were divided into three age groups. Group I: age
0-4 years. Group II: age 4-8 years and group III:
age 8-14 years.
Patients with high clinical suspicion and the
presence of clinical skin symptoms were included.
Confirmation of the diagnosis was based on the
positive microscopical examination.
Clinical symptoms were defined as generalized
skin itching increased at night associated with
scratching, excoriated papules, vesicles and burrows.
Patients presenting with localized skin itching
or itching increased at day and night, or with
no specific time of exacerbation or diagnosed
with other diseases were excluded. The diagnosis
was based on the patient's history with physical
and laboratory findings.
This study used the clinical examination (by the
presence of burrows or erythematous papular, vesicular,
pustular or bullous lesions associated with itching
and a positive family history) followed by microscopic
test to confirm the diagnosis. The symptoms of
scabies include intense itching (especially at
night) with irritation of involved skin with redness
and blisters formation. The skin irritation is
more likely to be seen in the areas between the
fingers and toes; around the wrists or navel,
in the folds of the elbow, armpit, belt-line,
abdomen, groin and the genital area. The head,
neck, palms, and soles of the feet are usually
spared, except in babies.
The mite infestation was confirmed using scraping
test. The sampling was carried out from the children
suspected to have scabies infestation and carried
out on the patients with pruritus, nodules, and
papular rash. The lesions are gently scraped to
remove the topmost skin cells and particles which
were preserved in oily material then were mounted
on the microscope slide. The skin particle samples
including adult mites were referred as positive
samples.
From a total of 5,430 children who were examined
and treated for different diseases, one hundred
and seventy five patients (3.2%) had itching in
addition to other symptoms; 30 were excluded because
they were diagnosed to have other diseases that
cause itching (chicken pox and measles) and the
remaining were diagnosed to have scabies. Distribution
by age groups is illustrated in Table 1.
Table 1: Demographics
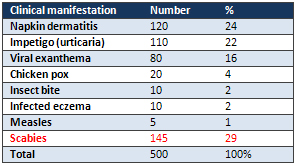
From the total 5,430; 500 patients presented with
different skin manifestations, 120 patients presented
with napkin dermatitis, 110 patients with skin
impetigo, 80 patients with viral exanthem due
to several viral infections, 20 patients with
chicken pox, 10 patients with insect bite reaction
(papular urticaria), 10 patients with infected
eczema and 5 patients presented with a picture
of german measles and rubeolla and 145 patients
were diagnosed by clinical examination and positive
microscopic test as scabies, Table 2.
Table 2: Common skin lesions seen in the clinic
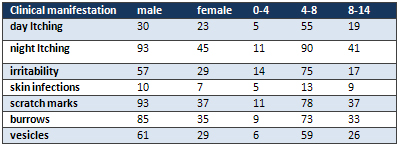
All scabies-infested patients presented with the
main complaint of itching; additional complaints
were irritability, skin infections, scratch marks
on skins. One hundred (69%) patients complained
of generalized itching especially at night and
45 (31%) of localized itching, Table 3.
Table 3: Clinical manifestations
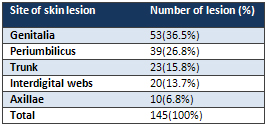
Commonest site for the scabies skin lesion was
genitalia in 53 (36.5%) patients, followed by
periumbilicus 39 (26.8%) patients, trunk 23 (15.8%)
patients, interdigital webs 20 (13.7%) patients
and axilla 10 (6.8%) patients, Table 4.
Table 4: Distribution of skin lesion
Scabies is a contagious disease caused by a mite.
The condition of 'scabies' is caused by an allergic
reaction to the fecal material of the mite Sarcoptes
scabei var hominus. It is an exceedingly common
disease of world -wide distribution. It is endemic
in many developing countries.
Although scabies is more common where overcrowded
conditions prevail, it can affect any individual
irrespective of social status, personal hygiene,
profession, gender, age or ethnic origin. It is
primarily characterised by itching, vesiculation
and pruritus. Signs of reddish, slightly elevated
tracts may also occur. Miniature papules, vesiculations,
pustules and excoriations soon appear. Scratching
of these areas may lead to secondary bacterial
infection. A recent review of the prevalence of
childhood skin diseases in developing tropical
and subtropical countries concluded that the prevalence
of scabies is in the range of 1-2%. (6)
Lice, Ringworm and Swimmer's itch, Measles and
Chickenpox, to mention a few can present with
itching. (7) These diseases must be differentiated
from scabies.
Scabies can be both one of the easiest and one
of the most difficult conditions to diagnose.
Scabies should be suspected in infants or children
with generalized pruritus of recent onset and
characteristic eruption. The site, severity, duration
and timing of the itch are all useful in the diagnosis.
Nocturnal itch is very characteristic of scabies.
A history of itching in other members of the family
should be sought and may give a clue to the diagnosis.
The classical eruption of scabies presents as
pruritic papules, vesicles, pustules and linear
burrows.(8) In our study the most frequent symptom
was night itching, followed by scratch marks and
burrows. Less common were secondary skin infection
and day itching.
In infants and young children, scabies often affects
the face, head, neck, scalp, palms, and soles.
Widespread eczematised erythema is common, particularly
on the trunk, and is sometimes more troublesome
than are lesions at typical sites. Very young
babies do not scratch and may just seem miserable
or feed poorly.(9) Genitalia and periumbilicus
were the commonest site of itching, although other
areas were affected (trunk, axilla and interdigital
webs) in the present study. Also the study showed
that the most common affected age group is between
4-8 years with male predominance.
The factors generally thought to explain the high
prevalence and incidence of common skin infections
in developing countries are poverty related and
include: a low level of hygiene, including difficulties
accessing water; climatic factors; and overcrowding
living conditions.(10, 11)
Scabies in our study is common and frequent because
of poverty, overcrowded living conditions, low
socioeconomic condition and poor hygiene. But
it is less common than in other countries and
communities. In remote Aboriginal communities
in Australia's Northern Territory, scabies is
endemic, with up to 50% of children and 25% of
adults infested at some times. (12) Prevalence
of scabies in African children can be as high
as 40-80%,(13) although a figure of 4.7% has been
reported in Nigerian school children. (14)
Scabies is a common health
problem among children
in Gaza; the disease can
be reduced by improving
socioeconomic, hygienic
conditions and by implementing
a proper system of social
education, as well as
by promoting a more efficient
health service. Work needs
to continue on addressing
these all-important factors
to bring about long-term
change.
1.
Water
related
diseases.
http://www.who.int/water_sanitation_health/diseases/scabies/en/
.
2.
Lapeere
H,
Naeyaert
J,
De
Weert
J,
De
Maeseneer,
Broche
L.
Incidence
of
scabies
in
Belgium.
Epidemiol
Infect.
2008;
136(3):
395-398.
3.
Walker
GJ,
Johnstone
PW.
Interventions
for
treating
scabies.
Cochrane
Database
Syst
Rev
2000;(3):
CD000320.
4.
McCarthy
JS,
Kemp
DJ,
Walton
SF,
Currie
BJ.
Scabies:
more
than
just
an
irritation.
Postgrad
Med
J
2004;
80:
382-7.
5.
Michael
J,
Graham
A.
More
common
skin
infections
in
children.
BMJ.
2005
May
21;
330(7501):
1194-1198.
6.
World
Health
Organization.
Epidemiology
and
management
of
common
skin
diseases
in
children
in
developing
countries.
Geneva:
World
Health
Organization;
2005.
p.
54.
7.
A
Quick
Guide
to
Common
Childhood
Diseases.
http://www.hlth.gov.bc.ca/prevent/phn.html
8.
Estes
SA.
Diagnosis
and
management
of
scabies.
Med
Clin
North
Am
1982;
66:
955-63.
9.
Meinking
TI,
Taplin
D.
Infestations
In:
Schachner
LA,
Hansen
RE,
editors.
Pediatric
Dermatology.
2nd
edition.
Churchill
Livingstone.
Edinburgh.
1995;
1347-1392.
10.
World
Health
Organization:
Epidemiology
and
Management
of
Common
Skin
Diseases
in
Developing
Countries.
Geneva,
World
Health
Organization;
2005.
11.
Haymann
DL:
Control
of
Communicable
Diseases
Control
Manual.
American
Washington,
Public
Health
Association
Press;
2004.
12.
Currie
BJ,
Carapetis
JR.
Skin
infections
and
infestations
in
Aboriginal
communities
in
northern
Australia.
Australas
J
Dermatol
2000;
144-5.
13.
Kristensen
JK.
Scabies
and
Pyoderma
in
Lilongwe,
Malawi.
Prevalence
and
seasonal
fluctuation.
Int
J
Dermatol
1991;
30:
699-
702.
14.
Ogunbiyi
AO,
Owoaje
E,
Ndahi
A.
Prevalence
of
skin
disorders
in
school
children
in
Ibadan,
Nigeria.
Pediatr
Dermatol.
2005;22:6-10.
|
|
.................................................................................................................

|
| |
|
