Enuresis
Nocturna and the Symptoms of Upper Airway Obstruction
in Primary School age Children: Is there a Relationship?
Doganer
Yusuf Cetin (1)
Aydogan Umit (2)
Ashfaq Tabinda (3)
Burmaoglu Serhat (4)
Sari Oktay (5)
Koc Bayram (6)
Saglam Kenan (7)
Qidwai Waris (8)
(1) MD, Department of Family Medicine, Mayo
Clinic and Foundation, Rochester, MN, USA.
(2) Assoc. Prof. Dr, Department of Family Medicine,
Gulhane Military Medical Faculty,
Ankara, Turkey.
(3) Assist. Prof. Dr, Department of Family Medicine,
Aga Khan University Hospital, Karachi, Pakistan.
(4) Assoc.Prof., Faculty of Economics and Administrative
sciences, Katip Celebi University, Izmir, Turkey
(5) Assist .Prof. Dr, Department of Family Medicine,
Gulhane Military Medical Faculty,
Ankara, Turkey.
(6) Prof. Dr, Department of Family Medicine,
Gulhane Military Medical Faculty, Ankara, Turkey.
(7) Prof. Dr, Department of Internal Medicine,
Gulhane Military Medical Faculty, Ankara, Turkey.
(8) Prof. Dr, Department of Family Medicine,
Aga Khan University Hospital, Karachi, Pakistan.
Correspondence:
DOGANER Yusuf Cetin, MD
Research Fellow, Mayo Clinic, Department of
Family Medicine,
Rochester, MN, USA
Turkish Military Academy Primary Care Examination
Center, Ankara, Turkey
GSM: +1 507 3190340
Email:
doganer.yusuf@mayo.edu , ycetindoganer@hotmail.com
|
Abstract
Objective:
Enuresis Nocturna (EN) associated with
symptoms of upper airway obstruction was
frequently observed in various studies.
In this study, EN associated with symptoms
of upper airway obstruction (breathing
problem while sleeping, sleep apnea syndrome,
sleeping with open mouth, snoring) was
examined.
Methods:
This study was conducted on 2314 students
between 6-14 years age, from 3 primary
schools in Ankara between January-May
2011. The questionnaires, questioning
EN and the symptoms of upper airway obstruction,
were distributed to students to be filled
in by parents.
Results:
The mean age of 2314 study participants
(1123 male, 1191 female) was 9.21 ±
2.08 (6-14 years). When students were
evaluated as groups with EN and without
EN, a statistically significant difference
was detected between groups regarding
upper airway obstruction symptoms (breathing
problem while sleeping, sleep apnea syndrome,
sleeping with open mouth and snoring)
(respectively p=0.002, p=0.036, p<0.001,
p<0.001). When students were examined
by dividing into 3 age groups as Group
I(6-8 age), Group II(9-11 age) and Group
III(12-14 age), a statistically significant
difference was detected between age groups
with EN (+), regarding breathing problem
while sleeping and sleep apnea syndrome
(respectively p=0.025, p=0.004).
Conclusion:
As was detected in this study, EN could
accompany upper airway obstruction symptoms
as was detected in this study. Thus, taking
a detailed medical history and physical
examination at the primary care centers
is significant.
Key words:
Nocturnal enuresis; airway obstruction;
child
|
The adenoids and tonsils in the upper airway are
very small at birth and then they grow during
the first 4 years of the life. They tend to shrink
toward the adolescence period (1). During this
period, children with adenoid and tonsillar hypertrophy
could show some pathological symptoms and signs.
It is stated that recurrent acute and chronic
inflammation cause adenoid hypertrophy in some
children (2). Adenoid and tonsillar hypertrophy
can cause serious diseases from snoring to Obstructive
Sleep Apnea Syndrome (OUAS), based on pharyngeal
obstruction and respiratory disorders while sleeping.
Snoring, mouth breathing, apnea and enuresis nocturna
(EN) are detected as the most frequently seen
symptoms during night (1).
It is found that EN during adolescence and childhood
period is related with obstructive respiratory
disorders occurring during night (3). EN can be
described as involuntary urination or urinary
incontinence of children above 5 during the night
(4). Enuresis is a clinical problem, which diminishes
the quality of life for children and their families.
Thus, children have emotional and learning-based
problems, which affect their social life (5).
It is detected that many children with enuresis
have a genetic susceptibility (6). In the studies,
it is stated that two possible physical disorders
could cause this situation. One of them is functional
bladder disorder while the other one is the maturational
delay in nocturnal arginine vasopressin secretion
(7).
The purpose of the study is to see the relationship
of EN with the symptoms of upper airway obstruction
in children at primary school-age.
Study design and subjects: This study was
a cross-sectional study and performed at 3, randomly
selected, primary schools in Ankara during January-May
2011. The counselor and school administrators
were informed about the details of study. A total
of 2500 students were approached for this study
through convenient sampling and around 2314 students
agreed to participate with a response rate of
92%.
Survey questionnaire: a pretested self-administered
questionnaire was used for data collection. A
Questionnaire was comprised of questions related
to socio-demographic characteristics of participants,
such as age, sex, income level, the education
level of parents, symptoms of upper airway obstruction
i.e.; breathing problem while sleeping, sleep
apnea syndrome, sleeping with open mouth, snoring
etc, and about their EN status. The participants
were also asked about frequency of being diagnosed
with recurrent upper respiratory tract infection
(URTI) and acute otitis media (AOM).
EN was described as urinary incontinence of
more than once a month in children above 5 years
old, without any related symptoms. EN can be
divided into primary EN (80%) and secondary
EN (20%). In primary EN, it is possible to have
lifelong urinary incontinence, while in secondary
EN; urinary incontinence begins after at least
six months of staying dry. In this study we
included patients presenting with primary enuresis
while patients with secondary enuresis were
excluded and student group with enuresis nocturna
was described as EN (+) and without enuresis
nocturna was described as EN (-). Sleep apnea
syndrome was evaluated as the most serious upper
respiratory tract obstruction symptom. The sleep
apnea syndrome was described as respiratory
arrest lasting more than 5-10 seconds during
sleep due to any reason. If apnea attacks happened
more than 4 times a week, it was described as
"during every sleep"; if it was 3-4
times a week, it was described as "frequently";
if it was twice a week, it was described as
"sometimes" and if it was once a week,
it was described as "rarely".
Ethical Approval: The parents of students
were informed about the study purpose and their
written consent was taken. Ethics approval was
taken from the ethical committee of Gulhane
Military Medical Academy (GMMA) (No:1491-941-09/1539)
and also necessary permission was obtained from
Ankara Provincial Directorate of National Education.
Statistical analysis: SPSS 15.0 for
Windows (Chicago-USA) package program was used
for evaluating the data obtained from the study.
Descriptive statistical methods were used to
state categorical variables in numbers and percentages,
and continuous variables in mean ± standard
deviation. Chi-square test was used to compare
discrete variables. While examining the upper
airway obstruction symptoms related with EN
in children in the sample group, logistic regression
analyses was performed by encoding EN (+) as
1 and EN(-) as 0. Calculation of odds ratios
(OR) for EN (+) group and 95% confidence intervals
(CI) were made using univariate logistic regression
model. The level of p< 0.05 was considered
significant.
A total of 2500 primary school-age children parents
were approached out of which 2314 completely filled
the questionnaire with a response rate of 92.56%.
The average age of study group was 9.21±2.08
with a male predominance; i.e. 5%.
For analysis purpose students were divided into
three groups; as Group I of 6-8 years old students
(n=958), Group II of 9-11 years old students (n=1014)
and Group III of 12-14 years old students (n=342).
The overall prevalence of EN for all students
was found to be 9.9% (n=230) in general. When
assessing prevalence in terms of age groups, the
rate of EN was 14.1% (n=135) for the students
of Group I, 8.1% (n=82) for the students of Group
II and 3.8% (n=13) for Group III (p<0.001).
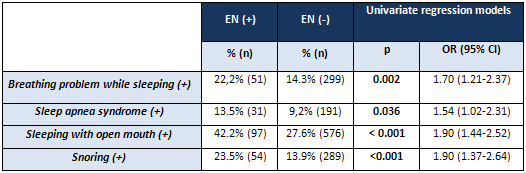
The frequency of upper respiratory tract obstruction
symptoms (breathing problem while sleeping, sleep
apnea syndrome, sleeping with open mouth, snoring)
in EN (+) and EN (-) groups are shown in Table
1. Sleep apnea was recognized as the most serious
upper airway obstruction symptom. In EN (+) group,
31 students had sleep apnea syndrome, the distribution
of them regarding the age groups was as follows:
12 students were in Group I and 19 students were
in Group II. The frequency of apnea attacks was
evaluated in EN (+) group; it was detected that
24 students had it "very rare", 2 students
had it "sometimes" and 5 students had
it "during every night".
Table 1: Comparison of upper respiratory tract
obstruction symptoms of students in EN (+) and
EN (-) groups
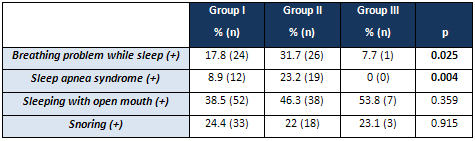
When the students with EN were evaluated regarding
age groups (Group I, II, III), a statistically
significant difference was determined between
groups, regarding breathing problem while sleeping
and apnea attack (respectively, p=0.025, p=0.004).
When the groups were evaluated regarding sleeping
with open mouth and snoring, there was not a statistically
significant difference (p>0.05) (Table 2).
Table 2: The comparison of upper airway obstruction
symptoms regarding age groups
We performed a logistic regression analysis
to determine the most effective discriminating
variable(s). Hence, we could see the most effective
variable(s) at the last step of the model. The
model coefficients were tested by omnibus test
and they were statistically significant (p<0.05).
In addition, according to Hosmer and Lemeshow
Goodness-of-Fit test the model is statistically
significant (Chi-Square=0.148; df =2; p>0.05).
When the relational statistics Cox & Snell
R Square and Nagelkerke R Square values are
seen, it could be interpreted that these statistics
were moderately low. It is known that there
are many other variables affecting EN in real
life; however we applied the model just for
four of them, so we evaluated these relational
values as acceptable. Finally the model with
variables and the statistics from them can be
seen in Table 3.
Table 3: Logistics regression model coefficients
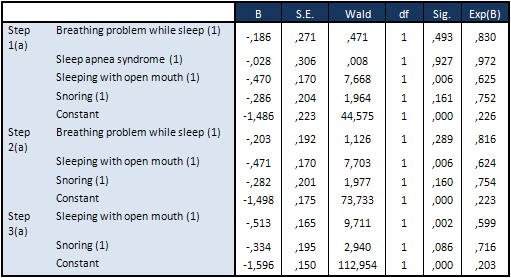
As seen in Table 3, "Sleeping with open
mouth" variable is statistically significant
for all steps. When we examine the third step,
"Sleeping with open mouth" (Wald=9.711;
p<0.05) and "Snoring" (Wald=2.940;
p<0.10) can be accepted as the most efficient
variables for EN (+) and EN (-) discrimination.
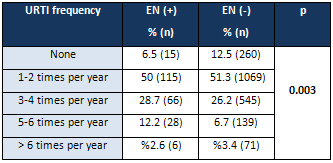
When EN (+) and EN (-) groups were evaluated
regarding the frequency of upper respairatory
tract infection, 12.2% of the students in EN
(+) group had URTI 5-6 times a year and this
rate was 6.7% in EN (-) group (p=0.003) (Table
4).
Table 4: Comparison of URTI frequencies in
EN (+) and EN (-) student groups
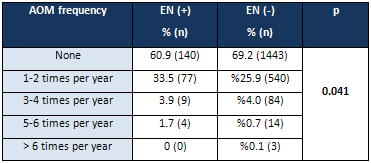
When EN (+) and EN (-) groups were evaluated
regarding recurrent acute otitis media (AOM),
33.5% of the students in EN (+) group had AOM
problem 1-2 times a year and this rate was 25.9%
in EN (-) group (p=0.041) (Table 5).
Table 5. Comparison of AOM frequencies in
EN (+) and EN (-) student groups
For the rate of students, who had surgical
operation due to upper airway obstruction symptoms
(tonsillectomy, adenoidectomy, adenotonsillectomy)
was 7.6% (n=175), the mean age of students was
5.71±1.83 (2-11 years old), when they
had the operation. 57.1% (n=100) of the students,
who had the operation, were male and 42.9% (n=75)
were female. The distribution of operations
was as follows: 10.9% (n=19) was tonsillectomy,
33.1% (n=58) adenoidectomy, 56% (n=98) adenotonsillectomy.
Even if the difference was not statistically
significant, 8.6% of the students, who had a
surgical operation related to upper airway obstruction,
had EN while this rate was 10.1% for students,
who did not have a surgical operation.
During childhood, there are many factors,
particularly adenoid and tonsillar hypertrophy,
which restrict air flow through the upper airway.
Adenoid and tonsillar hypertrophy is taken normally
during this period, when children have nasal
and throat infections frequently (1, 8). Enlarged
adenoids can block air flow through the nasal
cavity. This situation can result in snoring,
mouth breathing, and nasal speech (7). EN is
another clinic case, thought to develop during
this period as a result of upper airway obstructions.
In this study, it was detected that symptoms
of upper airway obstruction such as breathing
problem while sleeping, apnea attacks, sleeping
with open mouth and snoring were seen more frequently
in children with EN. When the children with
Enuresis were evaluated regarding the age groups,
it was detected that there was a difference
between groups regarding breathing problem while
sleeping and apnea attacks and it was determined
that this difference depended on the increasing
number of these two symptoms in Group II (9-11
years old) students.
There have been many studies demonstrating
the correlation between upper respiratory tract
obstruction and EN. In the study of Cinar et
al., it was found that the etiologic relation
between EN and upper airway obstruction was
stronger than estimated (9). Alexopoulos et
al. examined the relation between primary EN
during childhood and snoring. This study included
1821 students (5-14 years old) and it was determined
that 135 students (7.4%) had habitual snoring
(HS). As a result of this study, it was determined
that children with HS were diagnosed with primary
EN more frequently than children without HS
(3). In the study of Ersu et al, it was stated
that HS was a serious problem for children and
could be related with diurnal symptoms. The
study included 2147 primary school students
(5-13 years old) and it was detected that of
students with HS (7%) had apnea, restless leg
syndrome, parasomnia and nocturnal enuresis
more frequently than children without HS (10).
Ayd?n et al. examined EN and upper airway obstruction
symptoms, developed by adenoid hypertrophy and
1090 primary school students (5-14 years old)
were included in the study. When the students
were evaluated separately under 3 groups as
5-7 years old, 8-10 years old, 11-14 years old
students, contrary to the former studies, there
was no significant difference between groups
regarding the relation of EN frequency with
adenoid hypertrophy symptoms (7). In this study,
when sleeping with open mouth and snoring were
evaluated as the most simple symptoms of upper
respiratory tract obstruction, it was determined
that students with EN (+) had these problems
more frequently than students with EN (-). This
statistically significant difference between
groups supported the findings of former studies.
It was considered that the difference could
result from disorders in neuro-hormonal mechanisms,
which controlled urinary incontinence.
It was a frequently observed clinical finding
that sleep apnea syndrome was accompanied with
EN. In the study of Basha et al., 326 children
(2-18 years old), who had tonsillectomy or adenotonsillectomy,
were included and EN prevalence rate was detected
as 32.8% (n=107). After a period of 44 months,
it was detected during retrospective evaluation
that in 61.4% of the cases patients recovered
from EN completely, 22.8% EN was in remission
period and in 15.8% cases EN still existed (11).
In the study of Brooks and Topol, 160 children,
having breathing problem while sleeping, were
polisomnographically evaluated and also Respiratory
Disturbance Index (RDI) was performed. It was
detected that 66 (41%) of the children were
enuretic. As a result of the study, it was determined
that children with RDI>1 had higher risk
of enuresis than children with RDI< or =1.
This result also revealed that respiratory difficulties
while sleeping increased the risk of enuresis
(12). Weissbach et al. evaluated 161 children
(4-18 years old) polisomnographically and examined
EN in the post-adenotonsillectomy period. In
an evaluation performed after nine months from
the operation, it was detected that EN symptoms
dramatically decreased after adenotonsillectomy
operation in children with obstructive sleep
apnea (13). Firoozi et al. obtained similar
results (14). Weider et al determined that patients
recovered from enuresis after having adenotonsillectomy,
which treated chronic adenotonsillar hypertrophy
and airway obstruction (15). In this study,
it was determined that the rate of students,
having breathing problem while sleeping or apnea
attacks, was higher in EN (+) than in EN (-)
group. The results of this study supported former
studies. This statistically significant difference
between EN (+) and EN (-) groups could be related
to a weak control of the regulation of Antidiuretic
Hormone (ADH) release, especially related with
REM (Rapid Eye Movement) sleep, and an increased
release of atrial natriuretic peptide (ANP).
In this study, the frequency of recurrent
URTI and AOM was also examined in addition to
upper airway obstruction symptoms. A statistically
significant difference was detected between
EN (+) and EN (-) student groups, regarding
the frequency of recurrent URTI and AOM. Although
there has been no study that directly has examined
the relation of URTI and AOM with EN, it is
clear that eustachian tube dysfunction, especially
which which resulted from adenoid hypertrophy,
forms the basis for URTI and AOM (7). Therapeutic
effectiveness of adenotonsillectomy in enuretic
children, who applied due to obstructive sleep
apnea symptoms, was shown in a limited number
of studies (14, 16). As it was determined in
this study, the relation of pathologies, which
caused upper airway obstruction like adenoid
hypertrophy, with EN supported indirectly the
relation between EN and AOM. It was considered
that increase in frequency of URI and AOM in
the EN (+) group resulted from the infection,
which occurred due to air passages obstruction.
Study limitations: Upper respiratory
tract obstruction symptoms could be observed
in children without adenoid hypertrophy. For
example, these symptoms could be observed in
children with allergic rhinitis, septal deviation
or concha hypertrophy. However these pathologies
are more rarely observed than adenoid hypertrophy
in this age group. Not being able to make a
differential diagnosis in children with these
symptoms was one of the most important limitations
of this study. Moreover, enuretic children could
not be examined prospectively because of the
cross-sectional study design. Another limitation
of this study was that it could not be determined
whether the children, who had surgical operation
because of upper airway obstruction, recovered
from EN or not. Because of study design, adenoids
and tonsils size could not be measured by physical
examination.
EN is a serious disease that has a potential to
cause important problems in social life. The importance
of a detailed medical history and physical examination
at primary care centers is evident, because the
initial contact with patients begins in these
centers. As it was detected in this study, even
if EN seems to be a urological pathology, it is
observed that it accompanies upper airway obstruction
symptoms frequently (breathing problem during
sleeping, sleep apnea syndrome, open mouth sleeping,
snoring).
The authors thank all students, parents and teachers
for their participation in this study, and the
principals of the schools and Regional Director
of Education of Ankara who made this study possible
by approving and supporting the process.
1. Kara C.O., Ergin H.,
Kocak G., Kilic I., M.
Yurdakul M. Prevalence
of tonsillar hypertrophy
and associated oropharyngeal
symptoms in primary school
children in Denizli, Turkey,
Int. J. Pediatr. Otorhinolaryngol.
66 (2) (2002) 175-179.
2. Potsic W.P. Assessment
and treatment of adenotonsillar
hypertrophy in children,
Am. J. Otolaryngol. 13
(5) (1992) 259-264.
3. Alexopoulos E.I., Kostadima
E., Pagonari I., Zintzaras
E., Gourgoulianis K.,
Kaditis A.G. Association
between primary nocturnal
enuresis and habitual
snoring in children, Urology
68 (2) (2006) 406-409.
4. Van Gool JD, Nieuwenhuis
E, Ten Doeschate IO, Messer
TP, De Jong TP. Subtypes
in monosymptomatic nocturnal
enuresis. II, Scand. J.
Urol. Nephrol. Suppl.
202 (1999) 8-11.
5. Gur E, Turhan P, Can
G, Akkus S, Sever L, Guzeloz
S, et al. Enuresis: prevalence,
risk factors and urinary
pathology among school
children in Istanbul,
Turkey. Pediatr Int 2004;46:58-63.
6. Bailey J.N., Ornitz
E.M., Gehricke J.G., Gabikian
P., Russell A.T., Smalley
S.L. Transmission of primary
nocturnal enuresis and
attention deficit hyperactivity
disorder, Acta Paediatr.
88 (12) (1999) 1364-1368.
7. Aydin S., Sanli A.,
Celebi O., Tasdemir O,
Paksoy M., Eken M., Hardal
U., Ayduran E. Prevalence
of adenoid hypertrophy
and nocturnal enuresis
in primary school children
in Istanbul, Turkey. International
Journal of Pediatric Otorhinolaryngology
2008;72:665-668.
8. Kornblut A.D. Non-neoplastic
disease of the tonsils
and adenoids, in: Paparella
M.M., Shumrick D.A., Gluckman
J.L., W.L. Meyerhoff W.L.
(Eds.). Otolaryngology,
third ed., W.B. Saunders
Co., Philadelphia, 1991,
pp. 2129-2147.
9. Cinar U., Vural C.,
Cakir B., Topuz E., Karaman
M.I., Turgut S. Nocturnal
enuresis and upper airway
obstruction, Int. J. Pediatr.
Otorhinolaryngol. 59 (2)
(2001) 115-118.
10. Ersu R., Arman A.R.,
Save D., Karadag B., Karakoc
F., Berkem M., Dagli E.
Prevalence of snoring
and symptoms of sleep-disordered
breathing in primary school
children in
Istanbul, Chest 126 (1)
(2004) 19-24.
11. Basha S., Bialowas
C., Ende K., Szeremeta
W. Effectiveness of adenotonsillectomy
in the resolution of nocturnal
enuresis secondary to
obstructive sleep apnea.
Laryngoscope 115(6) (2005)
1101-1103.
12. Brooks L.J., Topol
H.I. Enuresis in children
with sleep apnea. J. Pediatr.
142 (5) (2003) 515-518.
13. Weissbach A., Leiberman
A., Tarasiuk A., Goldbart
A., Tal A. Adenotonsilectomy
improves enuresis in children
with obstructive sleep
apnea syndrome, Int. J.
Pediatr. Otorhinolaryngol.
70 (8) (2006) 1351-1356.
14. Firoozi F., Batniji
R., Aslan A.R., Longhurst
P.A., Kogan B.A. Resolution
of diurnal incontinence
and nocturnal enuresis
after adenotonsillectomy
in children. J. Urol.
175 (5) (2006) 1885-1888.
15. Weider D.J., Sateia
M.J., West R.P. Nocturnal
enuresis in children with
upper airway obstruction,
Otolaryngol. Head Neck
Surg. 105 (3) (1991) 427-432.
|

