|
|
 |
| ............................................................. |
|
|
| ........................................................ |
| From
the Editor |

|
Editorial
A. Abyad (Chief Editor) |
|
|
|
|
........................................................
|
Original
Contribution/Clinical Investigation
|
|
|
<-- Turkey / International -->
Enuresis
Nocturna and the Symptoms of Upper Airway Obstruction
in Primary School age Children: Is there a Relationship?
[pdf
version]
Doganer Yusuf Cetin, Aydogan Umit , Ashfaq Tabinda,Burmaoglu
Serhat, Sari Oktay Koc Bayram, Saglam Kenan,
Qidwai Waris
<-- Sri Lanka -->
Referral
communications: Bridging the gap between primary
care doctors and specialists
[pdf
version]
R.P.J.C. Ramanayake, A.H.W. de Silva, D.P. Perera,
R.D.N. Sumanasekera, K.M.S.
Lakmini, B.L.S. Ranasigh
Appendix:
Click here for a template Referral form
<-- Jordan -->
Sodium
Stibogluconate treatment for cutaneous leishmaniasis:
A clinical study of 43 cases from the north
of Jordan
[pdf
version]
Mamoun Mohammad Al-Athamneh, Hiathem Qasem Abu
Al-haija, Ra’ed Smadi, Ayman S. Qaqaa ,Heba
Ajlouni
|
|
........................................................ |
Medicine and Society
........................................................
Clinical Research and
Methods
.......................................................
Continuing
Medical Education
|
Chief
Editor -
Abdulrazak
Abyad
MD, MPH, MBA, AGSF, AFCHSE
.........................................................
Editorial
Office -
Abyad Medical Center & Middle East Longevity
Institute
Azmi Street, Abdo Center,
PO BOX 618
Tripoli, Lebanon
Phone: (961) 6-443684
Fax: (961) 6-443685
Email:
aabyad@cyberia.net.lb
.........................................................
Publisher
-
Lesley
Pocock
medi+WORLD International
11 Colston Avenue,
Sherbrooke 3789
AUSTRALIA
Phone: +61 (3) 9005 9847
Fax: +61 (3) 9012 5857
Email:
lesleypocock@mediworld.com.au
.........................................................
Editorial
Enquiries -
abyad@cyberia.net.lb
.........................................................
Advertising
Enquiries -
lesleypocock@mediworld.com.au
.........................................................
While all
efforts have been made to ensure the accuracy
of the information in this journal, opinions
expressed are those of the authors and do not
necessarily reflect the views of The Publishers,
Editor or the Editorial Board. The publishers,
Editor and Editorial Board cannot be held responsible
for errors or any consequences arising from
the use of information contained in this journal;
or the views and opinions expressed. Publication
of any advertisements does not constitute any
endorsement by the Publishers and Editors of
the product advertised.
The contents
of this journal are copyright. Apart from any
fair dealing for purposes of private study,
research, criticism or review, as permitted
under the Australian Copyright Act, no part
of this program may be reproduced without the
permission of the publisher.
|
|
|
| September 2014
- Volume 12 Issue 7 |
|
Referral
communications: Bridging the gap between primary
care doctors and specialists
R.P.J.C.
Ramanayake (1)
A.H.W. de Silva (2)
D.P. Perera (2)
R.D.N. Sumanasekera (2)
K.M.S. Lakmini (3)
B.L.S. Ranasigha (3)
(1) Senior Lecturer: Department of Family
Medicine, Faculty of Medicine,
University of Kelaniya, Sri Lanka.
(2) Lecturer: Department of Family Medicine,
Faculty of Medicine,
University of Kelaniya, Sri Lanka.
(3) Demonstrator: Department of Family Medicine,
Faculty of Medicine,
University of Kelaniya, Sri Lanka.
Correspondence:
Dr. R.P.J.C. Ramanayaka
Department
of Family Medicine, Faculty of Medicine,
University of Kelaniya, Sri Lanka
Tel: 0094 773308700
Email:
rpjcr@yahoo.com
|
Abstract
Introduction: In
the Sri Lankan health system there is
no system for registering a patient under
any health care provider and there is
no established referral and back referral
system in practice. Still there is communication
between primary care doctors and specialists
mostly through conventional letters. This
study was conducted to explore views of
specialists on the referral process of
the country.
Methodology: This
was a descriptive cross sectional study.
A self administered questionnaire based
on the data gathered in earlier qualitative,
explorative research was prepared to gather
data. A postal survey was conducted among
Specialists island wide.
Results:
1100 specialists were included in the
study and the response rate was 20%. Although
specialists expect a referral letter from
general practitioners they receive one
only around 50% of the occasions. They
were not happy with the quality of letters
and expected a comprehensive referral
letter. They were keen to reply but time
constraints (50%), lack of secretarial
support (36%) and perception that reply
will not reach the sender (31%) were obstacles
in replying. Continuous medical education,
use of structured referral forms and strengthening
training programs were suggested to improve
communications.
Conclusions
and recommendations: Specialists have
a positive attitude towards their professional
relationship with GPs and they should
be made aware of this and try to enhance
their communication with specialists.
There should be rectifiable measures in
the systems which facilitate coordination
and communication between the two parties
and then the referral process will become
meaningful and beneficial to all the stakeholders.
Key words:
Referral letters, communications, specialists,
general practice
|
Sri Lanka has its own unique health care provider
system. Similar to most countries in the world,
the Sri Lankan health system also consists of
three levels of care, the primary, secondary and
tertiary and the health services which are offered
by both the state and the private sector.(1) However
all citizens have access to healthcare in any
part of the island from either the state or the
private sector.
Although Sri Lanka has an extensive network of
health care institutions, there is no system for
registering a patient under any health care provider(2)
and also there is no established referral and
back referral system in practice in the private
sector.(3) Therefore patients are free to select
a doctor of their choice for a given ailment and
referrals to specialists are not always through
a generalist. This situation has given rise to
free movement of patients within and between primary,
secondary and tertiary care.(2) The state sector
has a referral system for administrative purposes,
the patient having to get a "chit" from
the outpatient department to get into a specialist
clinic.(3)
Thus there is no accepted referral system particularly
in the private sector and also there is no continuity
of care or accountability for a given patient's
health outcomes either in the state or in the
private sector.
Referral of a patient for services of a specialist
is an inevitable and essential aspect of primary
medical care. Even though there is no established
system, coordination of patient care with a specialst
goes on in practice. We need to work towards a
proper referral system to deliver better quality
patient care. In this background, research related
to the present position in referral consultations
will be of great value and we have carried out
research from different angles to contribute to
the existing data.
Looking at a proper referral system, shows
that during the process of patient referral,
good communication and coordination between
primary care doctors/general practitioners (GPs)
and specialists is essential to provide continuity
of care and proper follow up of a patient. The
three parties involved in the process, general
practitioners, specialists and the patients
have their own expectations from communications;
specialists expect information about the problem
to be addressed and adequate relevant details,
GPs expect a clear response regarding diagnosis
and management and patients expect information
about the diagnosis, treatment and follow up
requirements. When these expectations are unmet
GPs, specialists and patients end up dissatisfied
with the process.(4) Research also has shown
that there is great variation in the referral
patterns and rates.(5) Possible reasons for
this may be characteristics of the patient (age,
gender, social status, level of education, occupation),
pressure from and expectations of patients,
characteristics of the physician (age, gender,
length of practice, patient load, willingness
to deal with uncertainty) and access to specialists.(6)
In referring patients in Sri Lanka, communication
between GPs and specialists takes place mostly
through letters(3,7) although there are other
forms of communication such as mobile phones,
e-mails etc. Studies on patient referrals are
scarce and published research involving specialists
on referral communications are not available
in the country. As the specialists play a key
role in establishing a proper referral system,
it was decided to conduct an island wide study
among specialists to explore their views.
This was a descriptive cross sectional study.
To prepare the list of specialists serving in
government hospitals all the secondary and tertiary
care hospitals were contacted and the names of
specialists were obtained. Similarly key private
sector hospitals were also contacted and details
of specialists visiting those hospitals were obtained.
Specialists rarely contacted by a primary care
doctors, such as anesthetists, and microbiologists
were excluded from the study.
Self administered questionnaire was prepared to
explore views of specialists. This questionnaire
was formulated based on the data gathered in earlier
qualitative, explorative research conducted among
specialists by the authors.(7)
The questionnaire was piloted to assess the applicability
(comprehension, formulation and length of time)
and necessary changes were made. It was mailed
to all the specialists in the list with a covering
letter with a stamped envelope to return it.
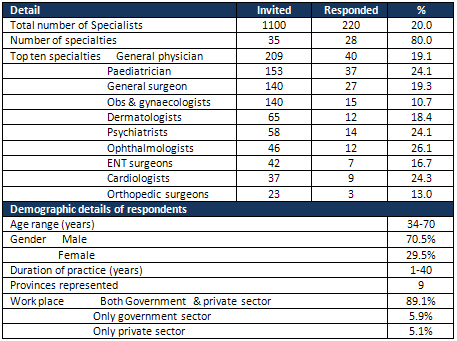
Table 1: Profile of specialists
Expectation and receiving of referral letters
Fifty five percent (55%) of the specialists always
expected a referral letter from a GP when a patient
was referred and the rest (45%) expected a letter
when important information had to be conveyed.
According to their perception only 3.7% receive
a letter always, while another 52.3% receive one
most of the time. 43.1% and 4.5% receive a referral
letter rarely and never, respectively.
Graph 1: Quality of referral letters
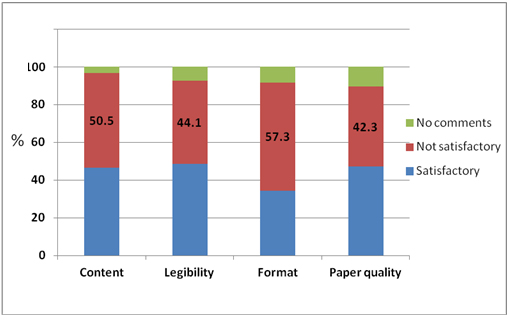
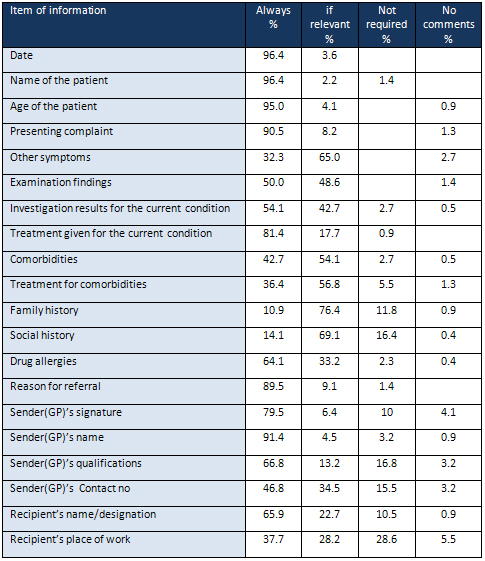
Table 2: Items of information expected by specialists
Replying to referrals
22.3% reply to referral letters always, 47.7%
respond most of the time while others (30%) reply
occasionally or rarely.
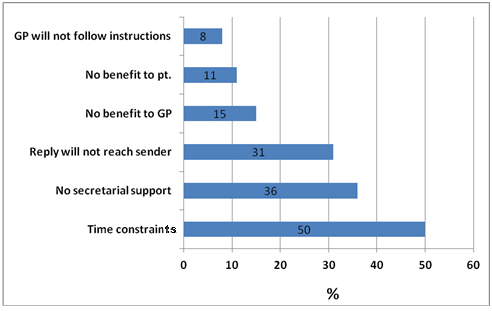
Graph 2: Reasons for not replying
Factors which influence specialists to write
a reply
The most important factor which influences a reply
was whether follow up was necessary (79.5%). Other
factors were type of condition (60%), quality
of referral (49.1%) and primary care doctor known
to the specialist (26.4%).
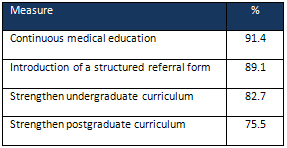
Table 3: Measures to improve the quality of referral
letters
This study sample included respondents from a
broad range of specialties from both the state
and the private sector heath care institutions
from all the provinces of the country. Thus, although
the response rate was only 20% it could be taken
as a representative sample.
The results show that 55% of the specialists expected
a referral letter from a GP always. The remaining
45% too indicated that they would be happy to
receive one if it conveyed relevant information
about the patient. However, this is contrary to
the results of studies that show the non provision
of a referral letter to the patient is due to
the GPs' perception that specialists and hospital
doctors are not keen to read their letters and
writing a comprehensive letter is a futile exercise.(8)
The experience of the specialists in this study
did not differ and almost 50% of them rarely or
never received a referral letter with referred
patients. Awareness about these findings among
the General Practitioners therefore may bring
about a change in their attitudes about referral
communications.
Specialists were unhappy with the quality of the
referral letters. Most of the doctors (57%) were
dissatisfied about the format of the referral
letters. Good format facilitates quick retrieval
of information and according to Rawal et al, format
contributes to comprehensiveness of letters as
well.(9) Letters were deficient in content as
well and perhaps unsatisfactory format could be
a contributory factor for omission of information.
Audit of referral letters in Sri Lanka also revealed
absence of important items of information in referral
letters(10) which confirms the opinion of specialists.
Legibility was also not satisfactory and it is
a futile exercise to write an illegible letter.
It's surprising that doctors have written letters
in substandard papers. It is evident from this
study that specialists are dissatisfied with the
quality of letters they receive and this could
create a negative opinion of GPs' work among specialists.(11)
Items of information expected by the specialists
show that they expect a comprehensive referral
letter from primary care doctors. More than 90%
of the specialists expected date, name and age
of the patient, reason for referral and GP's name
always. Name is the link between the patient's
identity and ensuing details which helps to avoid
medical errors. Date is the useful indicator of
the time duration and the progress of the condition
which enables proper evaluation of the patients'
condition and its progression. Reason for referral
shows the purpose of the referral. Other symptoms,
examination findings, investigation findings,
treatment tried, co-morbidities, treatment for
co-morbidities and drug allergies were expected
always or if relevant to the condition by more
than 90% of the specialists. Family history and
social history were expected only if relevant
to the patients' condition by the majority. It
shows that they do not expect a check list of
information for each and every patient but relevant
information for the particular patient. This finding
will be a guide for primary care doctors as to
what items of information should be included in
their referral letters.
For continuity of care to be maintained, it's
important that healthcare providers at all levels
of care remain informed of relevant information
pertaining to diagnosis, progress and management
plans for each of their
patients. Ideally all referred patients present
to a hospital or a specialist with a referral
letter which should return to the referring doctor
with a reply letter. Replies to referrals are
vital to enable comprehensive recording and follow
up care at primary care level as well. Although
70% of the specialists admitted that they reply
to referral letters always or most of the time,
this is contrary to the views of general practitioners.(12,13,14)
This interactive process should be balanced and
mutual and this will result only if both primary
care doctors and specialists respect each other.(6)
Several studies have revealed lack of respect
for GPs by specialists (8,15,16) and the Canadian
RESPECT study(15) suggested that this could be
improved by creating better relationships between
GPs and specialists, enhancing profile of family
medicine in Universities and teaching hospitals
and by changing negative attitudes by promoting
the expertise and role of family medicine. Specialists
may not understand the special work situation
in general practice where a doctor is usually
alone with a broad spectrum of clinical problems
and with minimal facilities.
Reasons pertaining to the work situation (Time
constraints and lack of secretarial support),
perceptions of health care system (reply letter
will not reach the GP) and impression that there
is no benefit to the patient or primary care doctor
were the key reasons for not replying to referrals.
Smith & Khutoane(17) also identified the same
reasons for not replying to referrals. In addition
they revealed poor quality referral letters, unnecessary
referrals, and the way services are structured
in hospitals also as contributory factors. Perhaps
the qualitative nature of that study allowed participants
more freedom to come out with a wide range of
issues.
The factors which influenced specialists to reply
to a referral were whether follow up of the patient
by the sender was necessary or not and the type
of the condition. Quality of the referral letter
also mattered for almost 50%. Lachman & Stander
revealed a correlation between the quality of
referral letters and reply rates.(18)
Although workload and time constraints were mentioned
as reasons for not replying, theoretically reply
letters could be a solution for that problem also.
A reply letter is an effective method of continued
education of GPs which in turn improves patient
care at primary care level leading to reduction
of the number of referrals and prevents unnecessary
referrals.(19)
Continuing medical education, undergraduate and
postgraduate training and using a structured referral
form for referrals were suggested by the specialists
to improve the quality of referrals. A practical
solution to improve the quality of letters would
be to use printed structured referral forms.(12,20,21)
Letter head will contain relevant details of the
sender while subheadings of the structured format
reminds information to be included, thus improving
the content. There will be a pre designed format
which would be a solution to unsatisfactory format
in conventional letters and also helps retrieval
of information by the recipient. A minimal number
of words needs to be hand written thus providing
an answer to illegible hand writing. If this letter
is printed on a standard paper it solves the problem
of using 'chits' to write referral letters.
| CONCLUSIONS
AND
RECOMMENDATIONS
|
• Specialists value
referral letters from
primary care doctors and
they expect a comprehensive
referral letter from primary
care doctors.
• They are not happy
with the quality of referral
letters.
• Specialists are
keen to reply to referrals
but work pressures and
deficiencies in the system
prevent them from replying.
• General practitioners
should be educated on
the importance and specialists'
attitudes towards referral
letters. Education programs
should strengthen and
continuous medical education
programs should be organized
to improve the quality
of referrals.
• Use of structured
referral forms should
be encouraged among GPs.
Appendix:
Click here for a template
Referral form, supplied
by the authors. It is
a Word version which you
can customise with your
own details
1.
Samarage
SM.
Migration
and
Human
Resources
for
Health:
From
Awareness
to
Action,
CICG
Geneva
23-24
March
2006.
2.
Ramanayake
RPJC,
Perera
DP,
De
Silva
AHW,
Sumanasekara
RDN.
Patient
held
medical
record:
solution
to
fragmented
care
in
Sri
Lanka.
theHealth
2013;4(3):51-57
3.
Karunarathna
L
De
A.
Consulting
wisely-an
art
in
family
medicine.
Sri
Lankan
Family
Physician
1999;22:8-15
4.
Piterman
L,
Koritsas
S.
Part
II.
General
practitioner-specialist
referral
process.
Intern
Med
J.
2005
Aug;35(8):491-6.
5.
O'Donnell
CA.
Variation
in
GP
referral
rates:
What
can
we
learn
from
the
literature?
Fam
Pract
2000;17:462-71
6.
Thorsen
O,
Hartveit
M,
Baerheim
A.
General
practitioners'
reflections
on
referring:
An
asymmetric
or
non-dialogical
process?
Scandinavian
Journal
of
Primary
Health
Care,
2012;
30:
241-246
7.
Ramanayake
RPJC,
Perera
DP,
De
Silva
AHW,
Fernando
KAT,
Athukorala
LACL.
Referral
communication
between
primary
and
secondary/tertiary
care;
views
of
specialists.
1st
national
conference
on
family
medicine
and
primary
care
April
2013,
New
Delhi,
India.
Abstract
book
:73.
8.
Gandi
TK,
Sitting
DF,
Franklin
M,
Sussman
AJ,
Fairchild
DG,
Bates
DW.
Communication
breakdown
in
the
outpatient
referral
process.
J
Gen
Intern
Med
2000;15:626-631
9.
Rawal
J,
Barnett
P,
Lloyd
BW.
Use
of
structured
letters
to
improve
communications
between
hospital
doctors
and
general
practitioners.
BMJ
1993;
307:
1044.
10.
Ramanayake
RPJC,
Perera
DP,
De
Silva
AHW,
Sumanasekara
RDN,
Jayasingha
LR,
Fernando
KAT,
Athukorala
LACL.
Referral
letters
from
general
practitioners
to
hospitals
in
Sri
Lanka;
Lack
information
and
clarity.
Middle
east
journal
of
family
medicine
2013;11(8):14-20
11.
Natanzon
I,
Ose
D,
Szecsenyi
J,
Campbell
S,
Roos
M,
Joos
S.
Does
GPs'
self-perception
of
their
professional
role
correspond
to
their
social
self-image?
a
qualitative
study
from
Germany.
BMC
Fam
Pract
2010;
11,
10.
doi:
10.1186/1471-2296-11-10
12.
Couper
ID,
Henbest
RJ.
The
quality
and
relationship
of
referral
and
reply
letters;
the
effect
of
introducing
a
pro-forma
letter.
S
Afr
Med
J
1996;
86:
1540-1542.
13.
Siddiqi
S,
Kielmann
A,
Khan
M,
Ali
N,
Ghaffar
A,
Sheikh
U,
Mumtaz
Z.
The
effectiveness
of
patient
referral
in
Pakistan.
Health
Policy
Plan.
2001
Jun;16(2):193-8
14.
Ramanayake
RPJC,
Perera
DP,
de
Silva
AHW,
Sumanasekera
RDN,
Jayasinghe
LR,
Fernando
KAT,
Athukorala
LACL.
Referral
letter
with
an
attached
structured
reply
form:
Is
it
a
solution
for
not
getting
replies.
Journal
of
Family
medicine
and
Primary
Care2013;2(4):
4.
15.
Manca
D,
Varnhagen
S,
Brett-Maclean
P,
Allen
GM,
Szafran
O.
Respect
from
specialists.
Can
Fam
Physician
2008;54:1434-5
16.
Fulton
J.
The
both
of
us.
Can
Fam
Physician
2011;57:525
17.
Smith
S,
Grace
Khutoane.
Why
Doctors
Do
Not
Answer
Referral
Letters
SA
Fam
Pract
2009;64-67
18.
Lachman
PI,
Stander
IA.
The
referral
letter.
A
problem
of
communication.
SAMJ
1991;79:98-100.
19.
Gagliardi
A.
Use
of
referral
reply
letters
for
continuing
medical
education:
A
review.
J
Contin
Educ
Health
Prof.
2002;22:222-9.
20.
Navarro
CM,
Miranda
IAN,
Onofre
MA,
Sposto
MR.
Referral
letters
in
oral
medicine:
standard
versus
nonstandard
letters.
Int
J
Oral
Maxillofac
Surg
2002;31:537-43.
21.
Jenkins
S,
Arroll
B,
Hawken
S,
Nicholson
R.
Referral
letters:
are
form
letters
better?
Br
J
Gen
Pract
1997;
47:
107-108.
|
|
.................................................................................................................

|
| |
|
