|
Perception of stress,
anxiety, depression and coping strategies among
medical students at Oman Medical College
Firdous Jahan
(1)
Muhammad A Siddiqui (2)
Mohammed Mitwally (3)
Noor Said Jasim Al Zubidi (4)
Huda Said Jasim Al Zubidi (4)
(1) Department
of Family Medicine, Oman Medical College, Sohar,
Oman
(2) School of Health Sciences, Queen Margaret
University Edinburgh, UK
(3) Head of Department of Psychiatry and Behavioral
Science, Oman Medical College, Sohar, Oman/
Faculty Mansoura University, Mansoura, Egypt
(4) Medical student. Oman Medical College, Sohar,
Oman
Correspondence:
Firdous
Jahan
Department of Family Medicine,
Oman Medical College, Sohar,
Oman
Email: firdous@omc.edu.com
|
Abstract
Objective:
To explore the stress sources, prevalence
of anxiety and depression and coping strategies
among preclinical and clinical under graduate
medical students.
Methods: A
cross sectional study was conducted on
Oman Medical College Students of pre-clinical
and clinical years. Data was collected
using Medical Student Stressor Questionnaire
(MSSQ), Hospital Anxiety and Depression
scale (HAD) and COPE questionnaire. Statistical
analysis was performed using SPSS (IBM
SPSS Statistics 20.0).
Results:
A total of 288 participants were enrolled
in which 123 were pre-clinical and 165
were clinical medical students. Nearly
two thirds (78.1%) of students were aged
between 20-24 years. Among all 87.5% (252)
were females and 12.5% (36) were males.
Collective score of academic stress factors
in the pre-clinical group was not statistically
different (p = 0.865) to the clinical
group. There was no significant difference
(P: 0.826; 95% CI: -3.511-2.804) in the
mean score of preclinical and clinical
group regarding Social Stress factors.
Coping strategies to control stress score
in the pre-clinical group was statistically
significantly (p < 0.001) higher than
the clinical group.
Conclusion:
The higher level of stress is associated
with poor academic performance, large
content of study material, exam and time
constraints. Coping strategies in students
were mainly better time management, emotional
support, talking to family members/friends
helps and good sleep relaxes them to control
stress.
Key words: Stress, coping stress,
medical students, anxiety, depression
|
The goal of medical education and curriculum
is to produce knowledgeable, skillful, competent,
safe and professional physicians. Some aspects
of medical education training and burden of
curriculum may cause some negative effects on
medical students’ mental and emotional
health[1]. Mental health wellbeing plays a significant
role in medical student’s career development
during study and has a significant impact on
the long-term health of doctors practicing in
different fields of the health care system[2].
Medical education is stressful and demanding.
Overwhelming burden of information, and lots
of competition to excel makes students anxious,
and nervous and with minimal opportunity to
relax and recreate [3]. Most students become
more active, creative, and productive because
of stress as it enables concentration for better
performance and energizes the person for hard
work. However, stress can cause significant
problems in student’s careers; prolonged,
uninterrupted, unexpected and unmanageable stress
is damaging [4]. Stress results when pressure
exceeds one’s perceived ability to cope;
it does not necessarily follow the presence
of a potential stressor. Academic stress is
a normal, desirable, and beneficial part of
our lives that can help one learn and grow.
However , stress is associated with depression,
drug abuse, anxiety and suicide [5-6]. Studies
suggest that student distress subsequently may
affect students’ care of patients, relationship
with faculty and family members, and ultimately
it can cause damage to the culture of the medical
profession[7-8].
Coping strategies are specific efforts that
individuals employ to manage stress, both behavioral
and psychological, so they can tolerate, reduce,
or minimize stressful events. Previous studies
show that coping plays a central role in adaptation
to stressful life events[9]. Literature has
reported the high incidence of stress in medical
students in different parts of the world. The
most common stressors among medical students
are high parental expectations, frequency of
examinations, vastness of academic curriculum,
sleeping difficulties, performance in periodic
examinations, and worries about the future[10]
. Stressors of medical students are generally
academic related stressors, interpersonal related
stressors, teaching and learning-related stressors,
and social related stressors. Therefore, early
detection of stressors among medical students
may prevent unwanted consequences on their health[11].
Oman Medical College (OMC) offers a seven-year
curriculum, leading to the degree of Doctor
of Medicine (MD). The College admits students
directly after their graduation from secondary
school. Students enter a one year General Foundation
Program. After successful completion of the
General Foundation Program, OMC students enter
a six-year MD Program. The MD Program entails
two years of premedical science studies, followed
by two years of basic biomedical science studies,
and culminates in two years of clinical training.
We conducted a study on medical students at
Oman Medical College regarding their perception
and recognition of stress and coping strategies.
A cross sectional study was carried out at
Oman Medical College in 2014 -15. Students of
pre-clinical and clinical years who consented
to participate in the study are included in
this survey.
Data Collection Tool/Survey Questionnaire:
Self-administered Questionnaire has 6 Sections:
I. Demography including age, gender, current
residence, family residence, family income,
family size, father and mothers’ education.
II. Academic stress factors : 0 no stress to
4 causing severe stress
III. Social stress factors: 0 no stress to 4
causing severe stress
IV. Coping strategies to control stress : 0=
Never done, 1=I have not been doing thi,s 2
= I’ve been doing this a little bit, 3
= I’ve been doing this a medium amount,
4 = I’ve been doing this a lot
V. Physical well being factors including somatic,
agitation, habits and chronicity : from 1-4
Strongly disagree to Strongly agree
VI. Hospital Anxiety and Depression scale (HAD)
Data was collected using Medical Student Stressor
Questionnaire (MSSQ) for academic and social
stress. This is a validated and reliable questionnaire
adopted with permission of the author. A number
of studies reported that reliability of six
constructs of the Medical Student Stressor Questionnaire
(MSSQ) ranged between 0.64 and 0.92, indicating
acceptable to high level of internal consistency.
Its validity and reliability was established
among medical students in different Malaysian
medical schools [12-14].
Hospital Anxiety and Depression scale (HAD);
the cut-off point of a score of 8 or more for
either the anxiety or depression components
denote possible anxiety and depression [14].
This cut-off point had a sensitivity of 0.89
and a specificity of 0.75 for the anxiety component
and a sensitivity of 0.80 and specificity of
0.88 for the depression component [15].
Coping strategies were assessed using the abbreviated
version of the COPE Inventory, a validated and
reliable instrument available online [16-17].
It is used to assess a broad range of coping
behaviors among adults with or without clinical
conditions. It consists of 19 items, and each
item is rated on a 4-point Likert scale ranging
from “I have not been doing this at all
(score 1)” to “I have been doing this
a lot (score 4)”. The higher score indicates
greater coping by the respondents. The items
are scored to produce different dimensions of
coping each reflecting the use of a coping strategy:
active coping, planning, acceptance, denial,
self-distraction, use of smoking, use of emotional
support, use of instrumental support, behavioral
disengagement, venting, positive reframing,
humor, religion, and self-blame.
The study protocol was approved by the ethical
review committee. All students in pre-clinical
and clinical years were invited to participate.
Participants were enrolled after taking written
informed consent. The principal investigator
ensured uniformity and two research assistants
trained participants how to fill it out. Validation
of the questionnaire on small pilot group was
also completed. Questionnaires were brought
back after being filled out and entered in the
database. All questionnaires were included in
the study, and there were no missing responses.
Data Analysis
Statistical analysis was performed using SPSS
(IBM SPSS Statistics 20.0). Data were expressed
in frequencies, mean and percentages. Cross
tabulation was performed to determine if there
was a relationship between subgroups. The chi-square
test for categorical data, t-test and Mann-Whitney
test were used to compare differences between
the two groups with parametric and non-parametric
continuous data for hypothesis testing.
A
total
of
288
participants
were
enrolled
in
which
123
/180
(68%)
were
pre-clinical
and
165/185(89%)
were
clinical
medical
students.
Nearly
two
thirds
(78.1%)
of
students
were
aged
between
20-24
years.
Among
all
87.5%
(252)
were
females
and
12.5%
(36)
were
males.
Majority
of
students’
family
(75.6%)
were
urban
residents
and
78.8
%
currently
resided
in
the
campus
accommodation
(Table
1).
Table
1:
Characteristics
of
Study
Participants
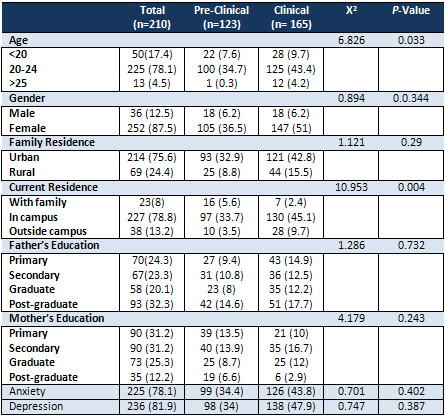
Participants
were
asked
multiple
questions
regarding
academic
stress
factors.
Their
answers
were
coded
from
1
to
5
where
1
is
not
stress
and
5
is
severe
stress.
The
most
frequent
responses
were
high
and
severe
stress
(74.3%)
during
tests/examinations
and
more
than
half
experienced
high
or
severe
stress
due
to
heavy
workload
(Table
2).
Collective
score
of
academic
stress
factors
in
the
pre-clinical
group
was
not
statistically
different
(p
=
0.865)
to
the
clinical
group.
Click
here
for
Table
2:
Student’s
response
on
Academic
Stress
Factors
Nearly
one
third
of
participants
feel
mild
stress
when
they
need
to
talk
to
patients
about
personal
problems
and
due
to
lack
of
time
for
socialization
with
friends.
More
than
a
quarter
(29%)
of
the
participants
feel
no
stress
secondary
to
verbal
or
physical
abuse
by
other
student(s),
and
26.2%
experienced
severe
stress
due
to
insufficient
time
for
family
(Table
3).
There
was
no
significant
difference
(P:
0.826;
95%
CI:
-3.511-2.804)
in
the
mean
score
of
preclinical
and
clinical
group
regarding
Social
Stress
factors.
Click
here
for
Table
3.
Student’s
response
on
Social
Stress
factors
More
than
one
third
of
students
38.9%,
36.1%,
41.3%
and
44.1%
pick
out
better
time
management,
emotional
support,
talking
to
family
members/friends
helps
and
good
sleep
relaxes
them
to
control
stress,
respectively.
Nearly
one
third
of
students
think
plan
things
ahead
(28.8%)
and
involve
in
religious
coping
reframing
(28.8%)
helped
them
a
lot
to
cope
with
stress
(Figure
1).
Coping
strategies
to
control
stress
score
in
the
pre-clinical
group
was
statistically
significantly
(p
<
0.001)
higher
than
the
clinical
group.
Figure
1:
Coping
Strategies
to
Control
Stress
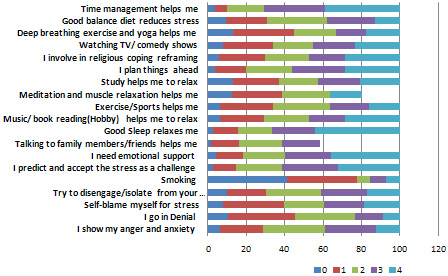
Where,
0=never
done
1=I
have
not
been
doing
this,
2
=
I’ve
been
doing
this
a
little
bit,
3
=
I’ve
been
doing
this
a
medium
amount,
4
=
I’ve
been
doing
this
a
lot
Students
were
asked
multiple
questions
regarding
health
problem
descriptions
in
the
past
year.
Their
answers
were
coded
into
strongly
disagree,
disagree,
agree
and
strongly
agree.
The
most
frequent
health
issues
are
headache,
backache,
bodyache
and
lack
of
appetite.
There
was
not
significant
difference
(p-0.878;
95%
CI-1.787-1.529)
observed
between
pre-clinical
(Mean-30.66±6.48)
and
clinical
(Mean-20.79±7.79)
group
score
regarding
health
issues.
Click
here
for
Table
4:
Health
Problems
descriptions
in
the
Past
Year
In
the
questionnaire,
students
were
asked
multiple
questions
regarding
how
they
have
been
feeling
in
the
past
week
(Table
5).
Their
answers
were
coded
into
most
of
time,
a
lot
of
time,
occasionally
and
not
at
all.
The
most
frequent
response
was
most
of
time
147
(51%),
106
(36.8%)
and
101
(35.1%)
for
laugh
and
see
the
funny
side
of
things,
look
forward
with
enjoyment
to
things
and
enjoy
a
good
book
or
program
respectively.
No
significant
difference
was
found
between
the
preclinical
and
clinical
groups
on
the
anxiety
and
depression
scores.)
Click
here
for
Table
5:
HAD
scale
The
main
goal
and
objective
of
medical
curriculum
is
to
provide
competent
and
safe
doctors
to
the
community
however,
there
are
few
aspects
of
medical
training
which
may
effect
medical
students’
mental
and
emotional
health
.
In
our
study
the
majority
are
female
students
and
their
families
are
living
in
urban
areas.
More
than
two
thirds
of
participants
are
living
in
a
campus
hostel.
Many
studies
in
the
western
countries
have
demonstrated
the
vulnerability
of
the
medical
students
to
psychiatric
disorders
[18].
Nearly
one
third
of
participants
of
our
study
feel
mild
stress
when
they
need
to
talk
to
patients
about
personal
problems
and
due
to
lack
of
time
for
socialization
with
friends.
They
feel
stressed
due
to
insufficient
time
for
family
as
well
as
facing
illness
or
death
of
the
patient.
The
majority
of
studies
on
stress
in
medical
education
focus
on
the
documentation
of
stress
and
information
on
the
correlates
of
stress
[19].
(Table
I)
Stress
and
health
issues
may
affect
medical
students’
academic
performance.
Student’s
stress
may
affect
care
of
patients,
relationship
with
faculty,
as
well
as
their
future
learning.
Coping
strategies
are
specific
efforts
that
individuals
employ
to
manage
stress
[20].
Stress
among
medical
students
is
a
great
concern
as
it
may
effect
on
behavior
of
students,
inhibition
of
learning,
and
ultimately
affect
patient
care
in
the
future
[21-22].
(Table
2)
The
negative
effects
of
long
and
tiring
medical
education
on
the
psychological
status
of
students
have
been
shown
in
several
studies[23-24].
Students
in
this
study
have
academic
stress
mainly
getting
poor
marks,
large
content
of
study
material,
exam
and
time
constraints.
Similar
results
are
reported
in
literature,
that
emotional
distress
and
academic
stress
is
the
top
most
finding
in
students
[25].
Appropriate
levels
of
stress
may
enhance
learning
in
medical
students,
however,
excessive
stress
might
cause
physical
and
mental
health
problems,
reduced
self-esteem,
and
may
affect
academic
achievement,
personal
and
professional
development
[26-27].
(Table
3)
In
Arab
countries,
epidemiological
research
about
psychiatric
morbidity
in
medical
students
is
uncommon.
Recently
performed
studies
showed
high
rate
of
anxiety
and
depression
in
undergraduate
medical
students
which
is
consistent
with
our
findings
in
this
study[28].
Nearly
one
third
of
students
think
plan
things
a
head
(28.8%)
and
involve
in
religious
coping
reframing
(28.8%)
helped
them
a
lot
to
cope
with
stress
(Figure
1).
Coping
strategies
to
control
stress
score
in
the
pre-clinical
group
was
statistically
significantly
(p
<
0.001),
higher
than
the
clinical
group.
Literature
shows
respecting
one’s
limits,
setting
priorities,
avoiding
comparisons
and
participating
in
leisure
activities
are
main
coping
strategies
[29-30].
Coping
strategies
in
this
study
showed
that
one
third
of
students
pick
out
better
time
management,
emotional
support,
talking
to
family
members/friends
helps
and
good
sleep
relaxes
them
to
control
stress
respectively.
As
reported
in
literature
the
stress
management
and
best
active
coping
strategies
are
to
maintain
a
well-balanced
academic
environment
for
improved
learning
experience[31].
(Fig
I)
Stress
can
lead
to
disruptions
in
both
physical
and
mental
health.
Self-reported
health
issues
in
our
studies
were
headache,
backache,
body
ache
and
lack
of
appetite.
Stress
induced
health
problems
if
excessive,
might
affect
academic
performance
and
professionalism
of
medical
students
[31-33].
(Table
4)
Stress
reduction
and
adopting
a
healthier
life
style
have
been
major
concerns
of
the
students
that
may
affect
their
learning
ability
and
academic
performance
[34-35].
In
our
study
HAD
scale
shows
significant
anxiety
level
in
medical
students
however,
there
is
no
difference
in
preclinical
and
clinical
students.(Table
5)
Stress
can
be
best
managed
by
regular
exercise,
meditation
or
other
relaxation
techniques,
structured
time
outs
and
learning
new
coping
strategies
to
handle
stress
in
medical
students
[36].
Identifying
stress
in
medical
students
early
in
their
pre-clinical
years
and
managing
appropriately
help
them
in
coping
with
stress
in
clinical
years.
This
is
imperative
to
get
academic
achievement
by
students
as
well
as
future
doctors’
professional
development
controlling
their
stress
and
anxiety
[37].
Oman
Medical
College
recognized
the
importance
of
students’
mental
health
and
emotional
integrity.
A
new
service
“Counselling
Center”
managed
by
the
department
of
Psychiatry
and
Behavioral
Science
for
students
has
been
established
by
Oman
Medical
College
in
year
2016.
Limitations
of
the
study:
This
is
a
cross-sectional
study
and
findings
of
this
study
are
based
on
self-reported
information
provided
by
students
which
can
have
some
bias
because
of
respondents’
interpretation
of
the
questions.
The
study
showed
a
diversity
of
stress
sources
and
stress
in
the
medical
students.
The
higher
level
of
stress
is
associated
with
poor
academic
performance,
large
content
of
study
material,
exam
and
time
constraints.
Coping
strategies
in
students
are
mainly
better
time
management,
emotional
support,
talking
to
family
members/friends
helps
and
good
sleep
relaxes
them
to
control
stress.
1.
Lamk
Al
Lamki.
Stress
in
the
Medical
Profession
and
its
roots
in
Medical
School.
SQU
Med
J,
April
2010;10(
1):
156-159.
2.
Mohd
Sidik
S,
Rampal
L,
Kaneson
N.
Prevalence
of
emotional
disorders
among
medical
students
in
a
Malaysian
university.
Asia
Pac
Fam
Med.
2003;2(4):213–217.
3.
Mehta
K,
Kaur
S,
Girgla
KK,
Kaur
P,
Kaur
H.
A
study
of
mental
distress
in
medical
students.
Natl
J
Physiol
Pharm
Pharmacol.
(2015).
5(3):
190-194.
doi:10.5455/njppp.2015.5.2810201415.
4.
Al
Riyami
A,
Attia
M,
Morsi
M,
Al
Kharusi
H,
Jaju
S:
Prevalence
of
mental
disorders
among
adolescent
secondary
school
Omani
students
and
their
utilization
of
Health
services.Results
of
the
World
Mental
Health
Composite
International
Diagnostic
Interview
Survey
2005.
Report
for
the
Ministry
of
Health,
Sultanate
of
Oman
2009.
5.
Stecker
T.
Well-being
in
an
academic
environment.
Med
Educ
2004;38:465-78.
6.
Moffat
K,
McConnachie
A,
Ross
S,
Morrison
J.
First
year
medical
student
stress
and
coping
in
a
problem
based
learning
medical
curriculum.
Med
Educ
2004;
38:482-91.
7.
Shapiro
S,
Shapiro
D,
Schwartz
G.
Stress
management
in
medical
education:
a
review
of
the
literature.
Acad
Med
2000;
75:748-59.
8.
Shah
M,
Hasan
S,
Malik
S,
Sreeramareddy
CT.
Perceived
stress,
sources
and
severity
of
stress
among
medical
undergraduates
in
a
Pakistani
medical
school.
BMC
Med
Educ.
2010;10:2.
9.
Sreeramareddy
CT,
Shankar
PR,
Binu
VS,
Mukhopadhyay
C,
Ray
B,
Menezes
RG.
Psychological
morbidity,
sources
of
stress
and
coping
strategies
among
undergraduate
medical
students
of
Nepal.
BMC
Med
Educ.
2007;7:26.
10.
Carver
C
S,
Connor-Smith
J.
Personality
and
coping.
Annu
Rev
Psychol,
2010;
61,
679-704.
11.
Singh
G,
Hankins
M,
Weinman
JA.
Does
medical
school
cause
health
anxiety
and
worry
in
medical
students?
Med
Educ.
2004;38:479–81.
12.
Muhamad
S.B.Y,
Ahmad
F.A.R
and
Yaacob
M.J.
The
development
and
validity
of
the
Medical
Student
Stressor
Questionnaire
(MSSQ),
ASEAN
Journal
of
Psychiatry,
Jan-June
2010;
11
(1).
Available
online:
http://www.aseanjournalofpsychiatry.org/oe11105.htm
13.
Muhammed
Saiful
Bahri
Yousuff.
A
multi-center
study
on
validity
of
medical
student
stressor
questionnaire(MMS).
International
Medical
Journal.
March
2011;18(1):14-18.
14.
Muhamad
Saiful
Bahri
Yusoff
A
confirmatory
factor
analysis
study
on
the
Medical
Student
Stressor
Questionnaire
among
Malaysian
medical
students,
Education
in
Medicine
Journal,
2011,
Vol.3
(1):
e44-e53
15.
Zigmond
AS,
Snaith
RP.
The
hospital
anxiety
and
depression
scale.
Acta
Psychiatr
Scand.
1983
Jun;67(6):361-70.
16.
Olssøn
I,
Mykletun
A,
Dahl
AA.
The
Hospital
Anxiety
and
Depression
Rating
Scale:
a
cross-sectional
study
of
psychometrics
and
case
finding
abilities
in
general
practice.
BMC
Psychiatry.
2005
Dec
14;5:46.
17.
Carver
CS.
You
want
to
measure
coping
but
your
protocol’s
too
long:
Consider
the
brief
COPE.
Int
J
Behav
Med.
1997;4(1):92–100.
18.
Abdulghani
HM.
Stress
and
depression
among
medical
students:
A
cross
sectional
study
at
a
medical
college
in
Saudi
Arabia.
Pak
J
Med
Sci.
2008;24(1):12–17.
19.
Zakiya
Al-Busaidi,
Kamlesh
Bhargava,
Aida
Al-Ismaily,
Hadia
Al-Lawati,
Rahma
Al-Kindi,
Mohammad
Al-Shafaee,
Abdullah
Al-Maniri.
Prevalence
of
Depressive
Symptoms
among
University
Students
in
Oman.
Oman
Medical
Journal
(2011)
Vol.
26,
No.
4:
235-239
DOI
10.
5001/omj.2011.58
20.
Lee
J,
Graham
A.
Students’
perception
of
medical
school
stress
and
their
evaluation
of
a
wellness
elective.
Med
Educ.
2001;35:652–9.
21.
Niemi
PM
and
Vainiomaki
PT.
Medical
students’
distress
-
quality,
continuity
and
gender
differences
during
a
six-year
medical
program.
Med
Teach,
2006;
28(2):
136-141.
22.
Sherina
MS,
Lekhraj
R
and
Nadarajan
K.
Prevalence
of
emotional
disorder
among
medical
students
in
a
Malaysian
university,
Asia
Pacific
Family
Medicine,
2003;
2:
213-217.
23.
Gholamreza
Sharifirad,
Abdoljalal
Marjani,
Charkazi
Abdolrahman,
Qorbani
Mostafa,
and
Shahnazi
Hossein.
Stress
among
Isfahan
medical
sciences
students.
J
Res
Med
Sci.
2012
Apr;
17(4):
402–406.
24.
Zaid
ZA,
Chan
SC
and
Ho
JJ.
Emotional
disorders
among
medical
students
in
a
Malaysian
private
medical
school.
Singapore
Med
J,
2007;
48(10):
895-899.
25.
Hamza
M.
Abdulghani,
Abdulaziz
A.
AlKanhal,
Ebrahim
S.
Mahmoud,
Gominda
G.
Ponnamperuma,
Eiad
A.
Alfaris
Stress
and
Its
Effects
on
Medical
Students:
A
Cross-sectional
Study
at
a
College
of
Medicine
in
Saudi
Arabia
J
Health
Popul
Nutr.
2011
October;
29(5):
516–522.
26.
Yusoff
MSB,
Rahim
AFA
and
Yaacob
MJ.
Prevalence
and
sources
of
stress
among
medical
students
in
Universiti
Sains
Malaysia,
Malaysian
Journal
of
Medical
Sciences,
2010;
17
(1).
|

