|
A case of Herlyn-Werner-
Wunderlic syndrome with recurrent lower abdominal
pain
Tariq Ertimeh
(1)
Rami AI-Shwyiat (2)
Khloud Mattar (3)
Rahmeh Adamat (4)
(1) MB BS, Senior specialist in obstetrics and
gynecology, reproductive endocrinology. King
Hussein Medical Centre, Amman, Jordan
(2) Consultant in obstetrics and gynecology,
urogynecology, King Hussein Medical Centre,
Amman, Jordan
(3) Senior specialist in obstetrics and gynecology,
King Hussein Medical Centre, Amman, Jordan
(4) RN, King Hussein Medical Centre, Amman,
Jordan
Correspondence:
Dr. Tariq Ertimeh
King Hussein Medical Centre,
Amman, Jordan
Email: tariqirtaimeh@gmail.com
Congenital anomalies of the Mullerian duct
system can result in various urogenital anomalies.
Herlyn -Werner- Wunderlich (HWW) syndrome is
a rare anomaly characterized by uterus didelphys
with blind hemivagina and ipsilateral renal
agenesis (1).
Mullerian duct anomalies have an incidence
of 2–3%. While obstructed hemivagina and
ipsilateral renal agenesis (OHVIRA) also known
as Herlyn Werner Wunderlich syndrome, constitutes
0.16–10% of these Mullerian duct anomalies
(11).
This syndrome was described for the first time
in 1922, and was suspected in a young woman
with regular menstruation and gradually increasing
pelvic pain and a pelvic mass formation, usually
noticed after menarche (2).
This anomaly is generally observed in post-menarche
adolescents and young women presenting as irregular
menstrual cycle, dysmenorrhea, abdominal pain,
and pelvic mass (3,4). It may also present with
urgency, frequency and vaginal discharge (12).
It is really difficult to achieve an accurate
diagnosis because menstruation is often regular
and when the patient complains of cyclic dysmenorrhea,
they are usually given anti-inflammatory drugs
and oral-contraceptives, thus causing a delay
in the diagnosis as they reduce or eliminate
menstrual blood. Also it may be attributed to
lack of understanding of this condition by radiologists,
gynecologists, and pediatricians.This may lead
to pelvic adhesions, endometriosis or infertility.
The experience with HWW syndrome was definitely
limited, consisting of case reports. It was
reported that laparoscopy is needed for accurate
diagnosis and treatment (5).
For diagnosis, ultra sonography usually gives
an accurate picture, by showing uterovaginal
duplication, hematocolpos or hematometrocolpos
along with the absence of ipsilateral kidney
(4).
However MRI has been considered as the imaging
modality of choice by various authors (6)
A 15-year-old girl presented with chief complaint
of lower abdominal pain during menses for last
6 months. Her menstrual history suggested no
abnormality except dysmenorrhea, she denied
any past medical or surgical history. One month
ago she presented to the emergency room complaining
of lower abdominal pain mainly on the right
iliac fossa with history of anorexia, nausea
and vomiting.
On examination secondary sexual characters
were normal for age. Abdominal examination showed
localized tenderness on the right iliac fossa;
rebound tenderness was positive. She was suspected
to have acute appendicitis versus ovarian torsion.
Appendectomy was performed and the histopathology
came back as normal appendix, the ovaries were
inspected intra-operatively; they were reported
as normal.
Two weeks later she has another attack of lower
abdominal pain. Ultrasound examination revealed
ovarian cyst (as reported by the radiologist)
and absent right kidney. She was referred to
the gynecologist for further assessment.
The patient was a virgin, thus vaginal examination
was not possible.
Ultrasonography was done which revealed double
uterus with hematocolpos and absent right kidney
with marked dilatation of the lower part of
the left ureter, while the left kidney was enlarged.
Congenital anomalies of the Mullerian duct
system can result in various urogenital anomalies
and Herlyn- Werner- Wunderlich syndrome is a
rare anomaly characterized by uterus didelphys
and blind hemivagina associated with ipsilateral
renal agenesis.
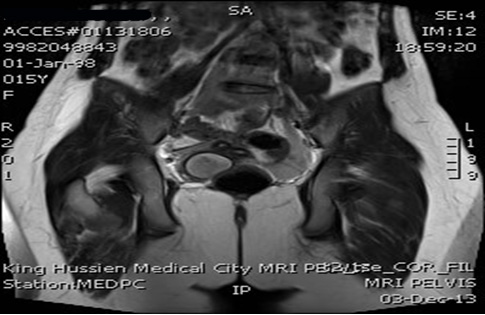
MRI imaging showed a utero-vaginal anomaly
consisting of didelphys uterus and double vagina,
one of which is obstructed and distended.
Figure 1: This MRI reveals double uterus
cavities, double cervix and absent right kidney
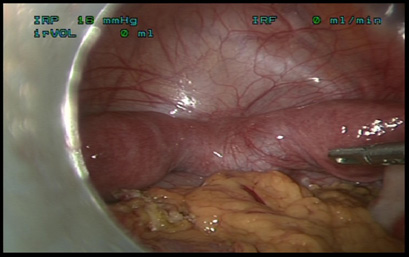
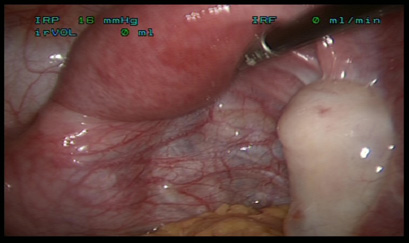
A few months later, diagnostic laparoscopy
was done for this patient which confirmed the
diagnosis.

This
patient
shows
how
it
is
difficult
to
diagnose
and
treat
such
uterine
malformations.
The
presence
of
acute
abdominal
pain
with
symptoms
like
those
of
acute
appendicitis
without
having
proper
ultrasound
done
by
experienced
radiologist
and
depending
only
on
clinical
picture
lead
to
unnecessary
surgical
intervention.
Our
patient’s
chief
complaint
was
pelvis
and
lower
abdominal
pain
with
dysmenorrhea.
The
symptoms
usually
begin
after
the
menarche.
Patients
with
this
syndrome
usually
menstruate
normally
and
may
have
no
specific
symptoms,
except
dysmenorreha.
Thus
20%
of
these
patients
are
diagnosed
in
their
20s
and
10%
are
diagnosed
beyond
age
30
years
(7).
Since
the
patient
presented
with
an
acute
abdomen,
appendicitis
and
ovarian
torsion
were
a
likely
possibility
following
trans-abdominal
ultrasound.
The
patient
was
taken
to
the
theater,
unnecessary
laparotomy
was
performed.
Could
more
accurate
diagnostic
imaging
have
prevented
the
emergency
intervention?
Transvaginal
ultrasound
might
have
revealed
the
underlying
disease
in
our
patient
which
was
hindered
by
her
virginity.
The
clinical
manifestations
and
physical
findings
are
very
helpful
to
diagnose
this
syndrome.
In
addition,
ultrasonography,
computed
tomography,
MRI,
and
exploratory
laparoscopy
are
used.
MRI
is
the
most
effective
method
and
helps
to
prevent
unnecessary
surgery
(8).
Ultrasonography
and
MRI
are
widely
and
effectively
used
in
the
diagnosis
of
genitourinary
anomalies,
a
100%
accuracy
being
reported
for
MRI
because
of
its
high
accuracy
and
detailed
elaboration
of
utero-vaginal
anatomy
(9,
10).
Transvaginal
excision
of
the
septum,
large
enough
to
allow
a
permanent
drainage
of
the
menstrual
blood
from
the
hemi-uterus
is
the
appropriate
mode
of
treatment
as
soon
as
the
condition
is
diagnosed.
The
family
of
our
patient
did
not
accept
doing
transvaginal
procedure
as
she
is
yet
single.
Regarding
their
concern
about
her
future
fertility,
they
were
reassured
that
women
with
uterus
didelphys
have
a
high
likelihood
of
becoming
pregnant
(13),
80%
are
able
to
conceive
(14).
At
last,
as
a
medical
clue
for
the
medical
team
if
a
young
patient
has
renal
anomaly
look
for
associated
vaginal
and
uterine
anomaly
this
may
help
an
early
diagnosis
(1)
Sarac
A,
Demir
MK.
Herlyn-
Werner-
Wunderlich
syndrome:
a
rare
cause
of
infertility.
Eur
Radiol
2009;
19:
1306-1308.
(2)
Lee
BH,
Kim
JW,
Oh
SI,
et
al.
3
cases
of
uterus
didelphys
with
obstructed
hemivagina
and
ipsilateral
renal
agenesis.
Korean
J
Obstet
Gynecol
1997;40:
1489-95.
(3)
Del
Vescovo
R,
Battisti
S,
Di
Paola
V,
et
al.Herlyn-Werner-Wunderlich
syndrome:
MRI
findings,
radiological
guide
(two
cases
and
literature
review),
and
differential
diagnosis.BMC
Med
Imaging
2012;
12:
4.
(4)
Vercellini
P,
Daguati
R,
Somigliana
E,
ViganoP,
Lanzani
A,
Fedele
L.
Asymmetric
lateral
distribution
of
obstructed
hemivagina
andrenal
agenesis
in
women
with
uterus
didelphys:
institutional
case
series
and
a
systematic
literature
review.
Fertil
Steril
2007;
87
(4):
719-24.
(5)
Zurawin
RK,
Dietrich
JE,
Heard
MJ,
Edwards
CL.
Didelphic
uterus
and
obstructed
hemivagina
with
renal
agenesis:
case
report
and
review
of
the
literature.
J
Pediatr
Adolesc
Gynecol
2004;
17:137-41.
(6)
Mirkovic
L,
Ljubic
A,
Mirkovic
D.
Magnetic
resonance
imaging
in
the
evaluation
of
uterus
didelphys
with
obstructed
hemivagina
and
renal
agenesis:
a
case
report.
Arch
Gynecol
Obstet
2006;
274:
246-247.
(7)
Candiani
GB,
Fedele
L,
Candiani
M.
Double
uterus,
blind
hemivagina,
and
ipsilateral
renal
agenesis:
36
cases
and
longterm
follow-up.
Obstet
Gynecol
1997;90:26-32.
(8)
Rana
R,
Pasrija
S,
Puri
M.
Herlyn-WernerWunderlich
syndrome
with
pregnancy:
a
rare
presentation.
Congenit
Anom
2008;48:142-3.
(9)
Troiano
RN,
McCarthy
SM.
Mullerian
duct
anomalies:
imaging
and
clinical
issues.
Radiology.
2004;
233:
19-34.
(10)
Prada
Arias
M,
Muguerza
Vellibre
R,
Montero
Sánchez
M,
Vázquez
Castelo
JL,
Arias
González
M,
Rodríguez
Costa
A.
Uterus
didelphys
with
obstructed
hemivagina
and
multicystic
dysplastic
kidney.
Eur
J
Pediatr
Surg.
2005
Dec;
15:
441-5.
(11)
Adair
L,
II,
Georgiades
M,
Osborne
R,
Ng
T.
Uterus
didelphys
with
unilateral
distal
vaginal
agenesis
and
ipsilateral
renal
agenesis:
Common
presentation
of
an
unusual
variation.
[Accessed
February
13,
2012];Journal
of
Radiology
Case
Reports.
2011
5:1–8.
http//
www.radiologycases.com/index.php/radiologycases/article/view/572.
[PMC
free
article]
[PubMed
(12)
Boram
H,
Herndon
C,
Rosen
M,
et
al.
Uterine
didelphys
associated
with
obstructed
hemivagina
and
ipsilateral
renal
anomaly
(OHVIRA)
syndrome:
Radiology
Case
Reports.
2010.
[Accessed
November
2,
2011].
http://radiology.casereports.net/index.php/rcr/article/viewFile/327/702
(13)
Güdücü
N,
Gönenç
G,
Içi
H,
Yiiter
AB,
Dünder
I.
Herlyn-Werner-Wunderlich
syndrome--timely
diagnosis
is
important
to
preserve
fertility.
J
Pediatr
Adolesc
Gynecol.
2012;25(5):e111-2.
[
Links
]
(14)
Heinonen
PK.
Clinical
implications
of
the
didelphic
uterus:
long-term
follow-up
of
49
cases.
Eur
J
Obstet
Gynecol
Reprod
Biol.
2000;91(2):183-90.
|

