Promoting
Self-Directed Learning in Family Medicine Residency
Program in Saudi Arabia
Mohammed H Doghether
Correspondence:
Dr.Mohammed H Doghether, MD
Family Medicine & Medical Education Consultant
Postgraduate Training Center
Ministry of Health
P.O.Box 90945,
Riyadh 11623
Kingdom of Saudi Arabia
Email: doghether@gmail.com
|
Abstract
This paper examined fostering self-directed
learning (SDL) in a residency program
in family medicine in Saudi Arabia. It
investigated the most effective ways to
help in appropriate application of Self-directed
learning in the residency program. Learning
is maximized when it is self-directed
so that residents study material that
is most relevant to them. Medical residents
learn best when they learn according to
their perceived needs and competency gaps
(learner-centered needs and gaps) which
are more beneficial than teacher-centered
ones. Residents engage in self-directed
learning by first identifying a clinical
problem, then pursuing the learning task,
next acquiring the new knowledge or skill,
and finally practicing the new knowledge
or skill. In this paper, I have described
a curricular intervention that employs
several educational and administrative
modalities to foster the self-direction
in learning in the family medicine training
program in Saudi Arabia.
Key words: medical education, family
medicine, residency program
|
"The only man who is educated is the man
who has learned how to learn" Carl
Rogers 1983
Although much of training in family practice addresses
the formal medical education, it is increasingly
believed that this is analogous to the tip of
iceberg, as it has been recognized that active
engagement in self-planned learning is more effective
than passive learning. The acquisition of self-directed
learning or Self Direction in Learning (SDL) skills
and the ability to keep up to date with development
in medicine are learning outcomes about which
there is a general agreement (1).
The Saudi Commission for health specialties (SCHS)
is the certifying and accrediting body for family
physicians and family medicine residency programs
in Saudi Arabia.
Saudi Board in family medicine consists of a four
year residency training program. The graduated
family physician is expected to be competent in
managing diseases, up-to date in terms of patient
care, and be responsible for his lifelong learning
in a world of rapidly changing and expanding knowledge
about treatment and investigations (2). In an
attempt to meet these challenges, the scientific
board of family medicine in SCHS has decided to
reform the residency program from the traditional
didactic teaching methods, to a competency-based
training program (2). One of the attractions of
competency-based CB curricula for reformers in
medical education is the potential to foster self-directed
learning as a lifelong habit. As has been mentioned
in studies (3), during implementation of the CB
program, it inconsistencies were found in the
interpretation of self-directed learning and its
importance in the residency program. Instead of
developing self-direction, students became overly
dependent on teacher instruction. The shift in
the conceptualization of self-directed learning
in CB Learning is obvious. The program is in need
of developing a conceptual framework to guide
teachers and students. The primary purpose of
the framework is to ensure that the goal of self-directed
learning, and its relationship to the other goals
of the residency program, are understood and interpreted
consistently, and in a way that is most likely
to achieve all goals effectively (4).
This paper explains the theories and principles
on which the framework, of the family medicine
residency program (FMRP) in Saudi Arabia is based.
SDL theories and principles:
Self-directed learning has been identified as
an important ability for medical graduates (4).
Malcolm Knowles established a definition of SDL
that guided work in this area. That definition
is:
A process in which individuals take the initiative,
with or without the help of others, in diagnosing
their learning needs, formulating goals, identifying
human and material resources, and evaluating learning
outcomes. (5).
This definition described learners as they move
linearly through a series of steps to reach their
learning goals.
Hammond and Collins developed in response to the
growth of the concept of SDL a more structured
definition:
A process in which learners take the initiative,
with the support and collaboration of others,
for increasing self-and-social-awareness; critically
analyzing and reflecting on the situations; diagnosing
their learning needs with specific reference to
competencies they have helped identify; formulating
socially and personally relevant learning goals,
identifying human and material resources for learning;
choosing and implementing appropriate learning
strategies, and reflecting on and evaluating their
learning. (6).
This definition views the SDL process as more
iterative, involving opportunities and interactions
in the environment, the personality characteristics
of learners, cognitive processes, the context
of learning, and opportunities to validate and
confirm SDL collaboratively. This definition forms
the basis for more recent models in SDL e.g. the
Personal Responsibility Orientation PRO by Hiemstra
(7).
In contrast to Self-directed learning; teacher-directed
learning is learning where the teacher chooses
what is to be learned, why it is to be learned
, how it is to be learned, where, when, and at
what level to be learned(4).
Among the bases for the self-directed learning
theory is the ability to change in practice, which
is known as reflective practice.
Reflective practice and learning from experience:
Patient centered education as well as learning
from experience were the most important reasons
as a basis for learning to change. Schon described
a cycle of learning from experience that incorporates
five stages (8, 9). An SDL approach is the most
applicable when the learner already has some relevant
knowledge and experience (4). While Kolb described
a four stage learning process called the experiential
learning theory (10).
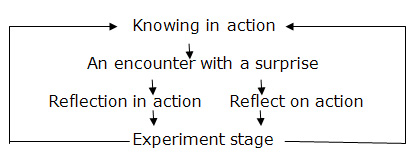
Schon cycle of reflective practice-(Adapted
from Prof Helen P Batty's lecture for Academic
Fellowship Program in 2006).
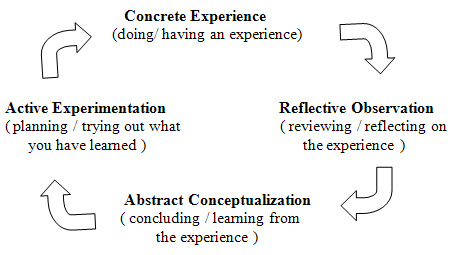
Kolb's learning cycle
The strengths of SDL:
The strengths of SDL in the field of medical education
are obvious; the following are summarized from
several sources:
• Student-centered learning; where the student
might not only choose what to study, but how and
why that topic might be an interesting one to
study. (11).
• Active learning; as adult learner, the
student will be active in the process of learning
where he will adopt deep approach to learning
(12).
• Meets the needs of individual learners;
learners have different needs and learn in different
ways. SDL is an approach which encourages the
learner's independency in the process of learning.
• Motivate the learner; as the learner becomes
more independent, responsibility for his learning
will be more; this in turn would increase his
interest in the program and his motivation as
a learner.
• Self-assessment; the learner will be encouraged
to do self-assessment. Self-assessment by the
learner will help him to recognize the gap in
his knowledge and skills which will determine
his learning needs.
• Self-learning skills; obviously SDL encourage
not only mastery of the content area being studied
but also the development of generic skills of
self-learning. Learning how to learn is an important
skill in continuing professional development (13).
• Constructivist approach-Students activate
prior knowledge and build on existing conceptual
knowledge frameworks (14).
• Outcome-based education; SDL is supported
by outcome-based education (curriculum) which
is considered more effective than process model
of curriculum.
• Cost effectiveness; SDL provides coherent
and effective learning strategy despite increasing
student numbers. Enable educators to supervise
larger numbers of learners. Repetition of frequently
taught materials can be avoided. Sharing of resources
between institutions will reduce the need to duplicate
resources. Saving time spent in formal education
will support the role of educator as a learning
facilitator.
The goal of self-directed learning in the
postgraduate program:
Lifelong learning is the goal of Self-directed
learning which Milflin (15) defined as the development
of physicians who:
• Are conscious of the need and accept
responsibility for evaluation of practice in
the light of changing understanding.
• Are able to identify deficiencies or
gaps in their own knowledge, skills and attitudes
(KSA).
• Are motivated to generate a learning
program to address deficiencies and fill the
gaps in KSA, including finding and using the
best evidence.
• Have the skills to identify, access and
use resources wisely and efficiently;
• Are able to evaluate learning efforts,
including resources used, and the effects on
practice, and
• Are committed to repeating the cycle
with each patient and clinical situation.
These skills meet the expectations of the SCHS
which are the skills needed for a competent
family physician.
Promoting SDL in residency program:
SDL is a comprehensive learning experience that
includes well-defined objectives, pre- and post
tests, and resources for accomplishing the objectives.
A model was developed to be a framework for
understanding self-direction in adult learning;
it consists of Personal Responsibility as a
Central Concept, Self-Directed Learning as The
Process Orientation, Learner Self-Direction
as The Personal Orientation, and Self-Direction
in Learning as The Vital Link. This model was
developed by Ralph G. Brockett and Roger Hiemstra(16),
which they refer to as the "Personal Responsibility
Orientation" (PRO) model of self-direction
in adult learning (illustrated below) which
is designed to recognize both the differences
and similarities between self-directed learning
as an instructional method and learner self-direction
as a personality characteristic (7). This model
is very interesting as it highlights the learner
importance in the process of SDL."The SDL
as a process focuses on characteristics of the
teaching-learning transaction. Thus, when considering
this aspect of self-direction, concern revolves
around factors external to the individual. Needs
assessment, evaluation, learning resources,
facilitator roles and skills, and independent
study are a few of the concepts that fall within
the domain of the self-directed learning process.
The learner self-direction, centers on a learner's
desire or preference for assuming responsibility
for learning. This is the personality aspect
discussed earlier. Thus, self-direction in learning
refers to both the external characteristics
of an instructional process and the internal
characteristics of the learner, where the individual
assumes primary responsibility for a learning
experience" (7). External factors and internal
factors (personality characteristics) lie under
the umbrella of the concept of Self Direction
in Learning. "The PRO model illustrates
this distinction between external and internal
forces. At the same time it recognizes, through
the notion of personal responsibility, that
there is a strong connection between self-directed
learning and learner self-direction" (7).
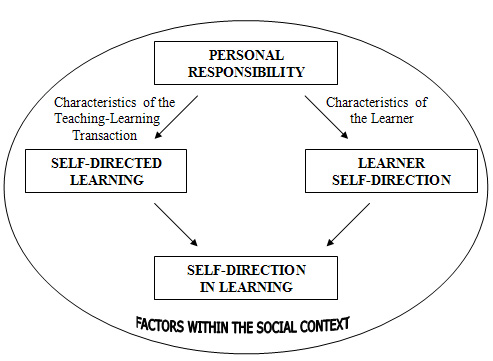
The "Personal Responsibility Orientation"
(PRO) Model. Reprinted with permission, Hiemstra,
R. (7).
Incorporating adult learning principles into
a predesigned educational package is challenging.
The solution might be through this model (PRO
model);
I. learner self direction
II. Self-directed learning as a process.
Learner self direction:
As mentioned above it deals with the personality
characteristics of the learner that affect his
survival in the self direction in learning.
Confidence is an essential component of SDL.
Teaching that builds confidence, such as providing
a supportive learning environment, supportive
teacher attitude, acknowledgement of various
learning styles and opportunities to practice
new skills in a variety of settings will enhance
the resident's self-concept as a competent learner
(17).
It is easiest when the learner already possesses
skills that facilitate SDL such as self-assessment
skills and library and informatics skills and
other skills, which will be mentioned later.
The SDL concept is somewhat not the usual strategy
in the training programs in Saudi Arabia, where
the learner has limited opportunities to assume
control of the learning process. The learners
in the training program need to develop fundamental
skills. Learners in our program (FMRP) need
to be trained in these skills:
• Self-assessment and identify their learning
needs.
• Information searching for the health
care literature and other databases
• Reading and critically appraising the
medical literature
• Clinical decision-making skills
These skills are preferably to be posed in the
early months of the program.
For the learners to develop these skills in
SDL, they need an intensive facilitation and
mentoring process by trained teachers. These
processes should be applied to the new learners
in the program (residents of first year R1).
Learners who are in advanced years might be
enrolled with the new residents orientation
to SDL skills if they are deficient in these
skills, otherwise if they have gained these
skills but are relatively inexperienced in SDL,
they might benefit from orientation short courses.
An example is one-month rotation in which they
learn informatics, critical appraisal, and clinical
decision-making skills. Residents are required
to apply these skills by critically assessing
a clinical practice of their choice. At the
end of the month, they formally present their
findings to an invited audience. Time is provided
within the curriculum for residents to work
on their projects.
SDL as a process:
Discussion groups promote active participation
in the learning process. Problem solving activities
such as case studies help the learners to validate
and use their experience as a learning source.
Working in groups is also believed to decrease
anxiety associated with lack of knowledge about
the topic (4).
During the first year of implementation of the
SDL in a PBL-curriculum, they found differences
of opinion among staff and students, and between
staff and students, about how to achieve the
goal (1). When the concept of self-direction
became counterproductive, dissonance about the
concept caused difficulties in the implementation
of the program. These difficulties might be
dealt with by preparing both teachers and students
to the process. Support to the student and teacher
through attending workshops preparing them to
identify their roles in the process of SDL would
help to minimize the inconsistency among the
educators and learners regarding the level of
input they were willing to give in relation
to SDL, which would be frustrating to both the
student and the teacher (18).
Development of self-directed modules requires
a substantial investment of time and work for
the teachers. The immediacy of giving the learner
an answer (pearls), spoon-feeding is quick,
but long term outcome is uncertain. Encouraging
the learner to find the answers will have advantages
of more student-teacher contact which will be
reflected positively on their relationship and
hopefully promote the process of SDL further
in terms of implementation.
Role of the Mentor:
According to the Society of General Internal
Medicine; mentoring is "a voluntary relationship
in which the mentor is usually an experienced,
highly regarded, empathetic individual, often
working in the same organization, or field,
as the mentee".
The Mentor role is significant as a contact
to and guide for the learner to foster the SDL.
Within the mentorship process, a mentor often
assumes multiple roles (19). The mentor may
be a role model, ensuring availability of resources,
and to provide the Learner with constructive
feedback. Mentor may be adviser, guide, listener,
coach, friend, or facilitator. The role that
best describes the mentor may be decided as
a result of how well the mentor understands
the total mentorship process. Clearly, the mentor
role does not suit all people, including professors
(20). This challenge needs us to train the mentors
through frequent accredited workshops as part
of continuing professional development CPD program
for the teachers (trainers). These workshops
must be SDL-based programs to help them learn
and understand how to apply SDL.
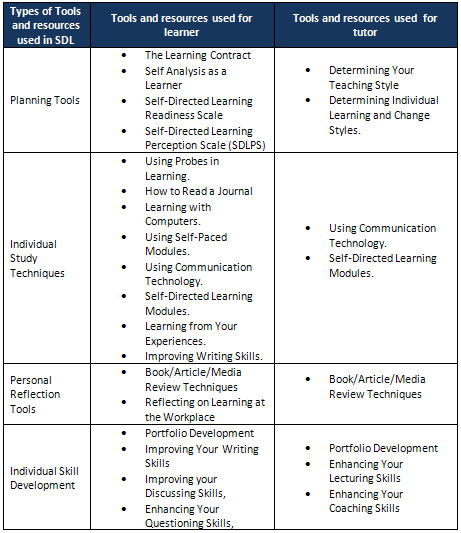
Tools and resources used in evaluation of
SDL:
Roger Hiemstra listed useful tools both for
learner and educator to help in the self direction
(see appendix B).
Difficulties in achieving the goal:
The ultimate result is the achievement of the
goal of self-direction in learning, but some
difficulties and barriers need to be addressed
and dealt with.
An important thing is that adult learners do
not always want to decide what to learn and
how to learn in an unfamiliar environment. Self-directed
learning may not be compatible with the learning
styles of our learners; especially most of them
lack the independent learning skills or have
not been oriented on previous experience in
undergraduate levels. The important result of
the dissonance was that students become frustrated,
struggling and many become dependent on direct
educator guidance (asking educator to tell them
what they would be assessed on).
As the learning is a change, and change may
be threatening, the student and teacher need
to feel secure and less threatened in the learning
environment to the extent to dare to experience
that which is new (20).
Lack of specific guidance and feedback to the
student and teacher is one of the major reasons
for the dissonance about the concept. This would
lead to further frustration causing anxiety
and distress for students. Feelings of frustration,
anger and anxiety could affect motivation. The
appropriate solution for this is through building
a positive supportive student-facilitator relationship.
Monthly half-day tutorials will help the students
to adopt the SDL in their learning where their
concerns and worries may be addressed.
Follow up on what learner actually searched
for, found, comprehended, and retained is often
sporadic and unsystematic. This can be solved
by educator assignments or learner's contract.
Challenges in the application of SDL:
The organizing committee for family medicine
in the Saudi Commission of Health Specialties
SCHS needs time and effort to recognize SDL
model for learning and to adapt the process
in the program in different training centres,
thereafter to evaluate its application.
This SDL as a process needs training of the
facilitators, mentors, students as well as teachers
to adopt the SDL. Arrangement of workshops is
costly to the individual training centers without
the support of SCHS. Two large workshops per
academic year per region (5 regions in Saudi
Arabia) might be more practical than more frequent
workshops.
As medical education is a new field in the country,
the numbers of those who can help in preparation
of the postgraduate training program to be SDL
based program are limited. Asking the help of
pioneers in this field from other countries
might be appropriate at least in the first few
years.
Although based on andragogical principles, the
modules may be presented in a pedagogical way,
thus promoting passive learning. The best way
to master the rudiments of a new area is to
be taught by an expert, at least at the beginning;
introducing them to the fundamental principles
and structures of SDL.
Self-directed modules may not be the best way
to address learning needs in all domains of
learning such as affective domain (4). Educators
need to behave ethically, which includes not
recommending a self-directed learning approach
if it is not congruent with the learners' needs.
Students become better self-directed learners
because of being in the curriculum for a longer
time, and, hence, becoming more experienced.
(15), which is an opportunity in our 4-years
program.
Miflin and his colleagues (15) published in
the next year to their previous study on application
of PB curriculum in undergraduate medical school
that in the light of the literature of higher
education and in the experiences of others in
problem-based medical curricula, the Learners
need support and guidance to foster the development
of self-directed, lifelong learning. Publishing
a guide for students to SDL, in which the general
educational principles are explained, enables
students to understand the nature and purpose
of the self direction in learning as a model.
This can be introduced in a thorough introduction
to the curriculum by means of orientation programs.
The roles of the teacher/preceptor in SDL:
Students will be assessed formatively over time
to ensure their development of skills to take
greater responsibility for directing their own
learning (21) including the foundation knowledge,
reasoning skills and confidence (15).
Miflin (15) described the tutor in SDL process
as:
initially model, then coach, and, as students
develop expertise in the process, the tutor
fades, intervening only where appropriate to
ensure students make optimal use of the case
for learning, and to ensure that they continue
to monitor the quality of learning.
In developing guidelines for educators, certain
points need to be addressed. The following list
summarizes points made by several writers (17)
regarding how adult educators can best facilitate
self-directed learning:
• Consider the student as an adult learner;
with the background as the traditional teacher-centered
learning as the student may be expected to have
pitfalls in their understanding of the SDL andthis
needs to be addressed in the guidance.
• Help the learner identify the starting
point for a learning project as it is new concept
for them.
• Help learners acquire the needs assessment
techniques necessary to discover what objectives
they should set.
• Learn and teach inquiry skills, decision
making, personal development, and self-evaluation
of work.
• Promote gradual independence of the student.
• Encourage the setting of objectives that
can be met in several ways and offer a variety
of options for evidence of successful performance.
• Develop a partnership with the student
by negotiating a learning contract for objectives,
methods, and evaluation criteria.
• Make sure that learners are aware of
resources and how to make use of them.
• Be a manager of the learning experience
rather than an information provider.
• Provide examples of previously acceptable
work (the minimal required). This will help
in relieving student's anxiety.
• Recognize learner personality types and
learning styles.
• Use techniques such as field experience
and problem solving that take advantage of adults'
rich experience base.
Role of educational institutions and employers:
The implementation of SDL will not be possible
and maintained without the involvement of educational
institutions and employers in providing SDL
experiences. Hiemstra R (7) recommends certain
points, the following:
• Conduct research on trends and learners'
interests.
• Obtain the necessary tools to assess
learners' current performance and to evaluate
their expected performance.
• Provide opportunities for learners to
reflect on what they are learning through half-day
tutorial every week.
• Encourage critical thinking skills by
incorporating such activities as seminars.
• Create an atmosphere of openness and
trust to promote better performance.
I would add these points to what Hiemstra mentioned
above:
• Promote Problem based small group learning.
• Promote inter-professional learning and
teaching.
• Have the program directors meet regularly
with panels of experts who can suggest curricula
and evaluation criteria.
• Help protect learners against manipulation
by promoting a code of ethics.
• Provide educators training on SDL.
• Provide a consult office for both educators
and students for the best ways to deal with
obstacles in application of SDL
• Conduct a 4 years-cyclical evaluation
of the program process and outcome.
Blended learning, defined as the combination
of traditional face-to-face learning and asynchronous
or synchronous e-learning. Blended learning
appears to have a consistent positive effect
in comparison with no intervention in health
professions (22).
All students should have access to the training
program Intranet and to the World Wide Web (23).
Resources specific to training program needs
are better provided in computer-based format
(e-blackboard) to allow time-independent access
for learners. Teachers should always be available
through the bulletin board on the intranet website
and by email. Those who are free can consult
with educator on an individual basis if necessary.
Later in the program, learners rely less on
educator-generated resources and use their patients
as primary resources for learning. Although
educators are encouraged to orient learners
to resources in clinical departments, the educator
is increasingly a role model and demonstrator
of clinical practice rather than provider of
factual knowledge and resources (15).
By
the
availability
of
resources
mentioned
above,
I
believe
that
the
first
year
learners
need
to
make
use
of
the
training
program
liaison
with
information
specialists
(librarians)
who
need
to
spend
considerable
time
coaching
learners
in
accessing
and
using
databases,
both
in
conventional
and
electronic
forms.
In
clinical
rotations
in
years
3
and
4,
learners
should
maintain
proficiency
by
applying
their
information
skills
in
evidence-based
practice.
Their
access
to
and
use
of
information
sources
is
increasingly
self-directed,
encouraged
by
and
modeled
on
the
practice
of
their
educators.
Methods
used
to
foster
SDL:
The
following
methods
have
been
mentioned
in
literature
as
a
practical
tips
for
self
direction
in
learning
which
are
good
to
be
used
to
foster
the
implementation
of
SDL
in
our
program:
Targeting
learner-specific
needs.
The
claim
that
there
is
never
enough
time
to
teach
everything
about
a
clinical
case,
especially
in
outpatient
teaching
is
no
longer
valid
with
one
minute
perception
(OMP)
as
the
teacher
can
know
what
is
the
learner's
greatest
need
or
deficit
on
a
particular
case.
OMP
is
very
helpful
and
perceived
by
residents
as
a
good
tool
in
family
medicine
teaching
sessions
(24).
Assignments.
This
is
where
a
clinical
question
is
identified
during
routine
patient
care
by
either
the
teacher
or
the
student.
The
teacher
will
ask
the
student,
or
group
of
students
to
find
related
information
that
help
in
answering
the
question
and
report
back
to
the
teacher,
group,
or
a
class.
These
assignments
need
to
increase
as
the
student
becomes
more
familiar
with
information
gathering
skills.
Volunteerism:
A
day
per
week
will
be
assigned
for
volunteerism
where
student
or
group
of
students
independently
identify
a
common
need
and
search
the
answers
which
will
help
to
adapt
the
reflective
practice.
This
might
be
fostered
further
when
the
teacher
can
be
a
role
model
and
practices
some
reflective
practice
in
the
teaching
session
with
the
students.
Dissemination
of
knowledge:
As
a
result
of
the
above
two
methods,
I
find
dissemination
of
knowledge
by
and
among
the
students
will
foster
implementation
of
SDL.
This
can
be
achieved
by
student
medical
journal
recognized
by
SCHS
where
publication
in
this
journal
is
considered
extra
credit
to
the
students.
Learning
contracts
LC:
the
first
step
in
developing
a
positive
student-teacher
relationship
is
when
a
student
and
teacher
agree,
at
the
beginning
of
a
rotation,
on
particular
learning
goals
and
come
up
with
a
plan
for
monitoring
and
evaluating
progress.
Students
need
help
from
the
teacher
on
how
to
develop
a
LC.
One
day
workshop
for
the
teachers'
refreshment
on
LC
might
be
needed
in
the
beginning
of
SDL
implementation.
(25)
As
the
LC
is
a
dynamic
in
its
nature,
changing
as
the
learner
progresses
in
the
learning
process,
the
student
will
fill
the
LC
with
the
help
of
the
teacher
and
mentor,
where
it
will
be
reviewed
every
three
months
for
the
1st
two
years
(R1
and
R2),
to
adopt
changes
as
the
students
progress
in
the
program,
then
every
year
for
the
2nd
two
years
(R3
and
R4).
Reporting
back.
Students
will
periodically
(at
every
quarter
of
the
rotation)
report
back
to
the
teacher
what
they
found.
This
is
through
a
written
format
(log
book,
brief
outline
or
1-page
handout,
etc.).
In
this
method
the
students
will
be
asked
to
report
back.
It
facilitates
evaluation
of
the
learner,
and
requires
the
learner
to
critique,
integrate,
and
present
information.
Feedback
from
the
site
of
the
teacher
is
important
to
help
student
improvement.
Resources:
Where
does
the
learner
find
information
and
answers?
The
program
will
offer
standard
textbooks
,
library
electronic
access
(for
medical
literatures),
electronic
black
boards
or
e-learning
software
platform
like
moodle
e-learning
platform
(MEP)
which
enables
educators
to
create
online
courses
to
encourage
interaction
and
collaborative
construction
of
learning
content.
It
provides
several
opportunities
for
the
'teacher'
to
transform
from
being
'the
source
of
knowledge'
to
being
a
facilitator
and
role
model
in
the
process
of
acquiring
knowledge
and
skills
(26).
As
computers
become
more
universally
incorporated
into
clinic
workstations,
they
will,
in
all
probability,
become
the
predominant
resource.
Portfolios:
A
portfolio
is
a
collection
of
products
prepared
by
the
student
that
provides
evidence
of
learning
and
achievement
related
to
a
learning
plan.
A
portfolio
typically
contains
written
documents
but
can
include
video
or
audio-recordings,
photographs,
and
other
forms
of
information.
Students
will
be
instructed
to
reflect
upon
what
has
been
learned
as
this
is
an
important
part
of
constructing
a
portfolio.
In
addition
to
products
of
learning,
the
portfolio
can
include
statements
about
what
has
been
learned,
its
application,
and
remaining
learning
needs
(27).
Mentor
would
help
student
in
identifying
remaining
learning
needs
and
how
they
can
be
met.
Portfolio
will
include
a
log
of
clinical
procedures
performed
during
training
program;
a
summary
of
the
research
literature
reviewed
when
selecting
a
treatment
option;
a
quality
improvement
project
plan
(e.g.
Audit
project),
and
report
of
results;
ethical
dilemmas
faced
and
how
they
were
handled;
a
computer
program
that
tracks
patient
care
outcomes;
or
a
recording
or
transcript
of
counseling
provided
to
patients.
Portfolio
can
be
a
paper
work
or
electronic.
The
electronic
one
is
very
easy
to
design
and
practice
with
a
lot
of
editing
features,
which
I
have
practiced
in
the
U
of
T
e-blackboard.
Portfolios
will
be
used
for
both
formative
and
summative
evaluation
of
students.
Portfolios
will
be
used
for
evaluating
mastery
of
competencies
that
are
difficult
to
evaluate
in
other
ways
such
as
practice-based
improvement,
use
of
scientific
evidence
in
patient
care,
professional
behaviors,
and
patient
advocacy.
Teaching
experiences,
morning
report,
patient
rounds,
individualized
study
or
research
projects
are
examples
of
learning
experiences
that
portfolios
will
be
most
useful
to
assess
them.
The
Royal
College
of
Physicians
and
Surgeons
of
Canada
in
the
Maintenance
of
Competence
Program
(MOCOMPS)
has
developed
a
portfolio
system
for
recertification
using
Internet-based
diaries
called
PCDiary©
that
could
be
adapted
to
residency
evaluations
(28).
Practice
based
small
group
learning:
the
evidence
is
supporting
the
use
of
Practice-Based
Learning
(PBL)
as
an
effective
method
for
teaching
under-graduates
in
medical
schools
and
used
more
and
more
in
Continuous
Professional
Development
(CPD)
activities
(29).
The
research
proves
the
PBSGL
effectiveness
in
postgraduate
teaching.
(30,
31)
In
the
adult
learning
theory,
adults
learn
best
when
they
are
required
to
address
problems
and
learning
is
maximized
when
it
is
self-directed
so
that
adults
study
material
that
is
most
relevant
to
them.
Clinicians
engage
in
self-directed
learning
by
first
identifying
a
clinical
problem,
then
pursuing
the
learning
task,
next
acquiring
the
new
knowledge
or
skill,
and
finally
practicing
the
new
knowledge
or
skill.(32)
In
this
paper,
I
have
described
a
curricular
intervention
that
employs
several
educational
and
administrative
modalities
to
foster
the
self
direction
in
learning
in
family
medicine
training
program
in
Saudi
Arabia.
The
program
should
be
designed
to
incorporate
principles
of
adult-learning
theory.
The
program
should
contain
exercises
to
enhance
skills
for
assessing
learning
needs,
developing
flexible
short-
and
long-term
learning
plans,
and
asking
and
answering
clinical
questions
efficiently.
I
sought
to
characterize
the
effects
of
this
teaching
program
on
physicians'
self-reported
learning
behaviors
and
self-efficacy
for
performing
essential
self-directed
learning
behaviors.
Appropriate
support
at
appropriate
intervals
means
that,
over
time,
students
are
motivated
and
enabled
to
guide
their
own
efforts,
secure
in
the
knowledge
that
they
have
developed
the
skills
and
attributes
which
will
allow
them
to
continue
learning
which
is
effective.
Increasingly,
instructional
methods
(PBL,
SDL,
EBM)
are
viewed
as
complementary
rather
than
exclusive
models.
Didactic
and
teacher-centered
teaching
probably
still
has
a
role,
even
as
other
instructional
strategies
are
utilized.
"Blended"
teaching
strategies
rather
than
predominant
teaching
strategies
are
increasingly
being
promulgated.
1)
Schostaka
J,
Davisb
M,
Jacky
Hansonc
J,
Schostakd
J,
Browne
T,Starkeg
PD,
Jenkinsh
N.
The
Effectiveness
of
Continuing
Professional
Development.
A
report
prepared
on
behalf
of
College
of
Emergency
Medicine,
Federation
of
Royal
Colleges
of
Physicians
and
Manchester
Metropolitan
University
,
2010.
2)
Saudi
Commission
for
Health
Specialization
SCHS
(2016).Saudi
Board
for
Family
Medicine-Manual
for
training
in
family
medicine.
Retrieved
November
3
,2016,
http://scfhs.info/Issues/
3)
Abu
Zuhairah
A,
Al-Dawood
K,
Khamis
A.
Family
medicine
training
in
Saudi
Arabia:
Are
there
any
variations
among
different
regions?.
Med
Edu.
2015;
(22);2:
106-110.
4)
Murad
MH,
Varkey
P
.
Self-directed
Learning
in
Health
Professions
Education
.
Ann
Acad
Med
Singapore.2008;37:580-90
5)
Knowles
MS.
Self-Directed
Learning
.A
guide
for
learners
and
teachers.
New
York,
NY:
Associated
Press;1975.
6)
Hammond
M
and
Collins
R.
Self-Directed
Learning;
Critical
Practice.
1991,
reprinted
2004.RoutledgeFalmer
ISBN
0-7494-0299-7.
7)
Hiemstra,
R.
Lifelong
learning:
An
exploration
of
adult
and
continuing
education
within
a
setting
of
lifelong
learning
needs
(Chapter
7
Theoretical
bases
and
research
in
adult
education)
(Third
Edition).
Fayetteville,
NY:
HiTree
Press;2002.
Retrieved
November
3,
2016,
http://www-distance.syr.edu/lllch7.html
8)
Schon
D.
The
reflective
practitioner.
1983;
New
York,
NY:Basic
Books.
9)
Schon
D.
Educating
the
reflective
practitioner.
1987;San
Francisco,Calif:Jossey-Bass
Publishers.
10)
Kolb
DA.
Experiential
Learning:
Experience
as
a
source
of
learning
and
Development.
Englewood
Calif,NJ:Prentice-Hall;
1984.
11)
O'Neill,
G.,
Moore,
S.,
McMullin,
B.
Dublin:
AISHE,
Emerging
Issues
in
the
Practice
of
University
Learning
and
Teaching..Released
under
Creative
Commons
licence:
Attribution-NonCommercial
.2005;
2.0.
Some
rights
reserved.
http://www.aishe.org/readings/2005-1/
12)
MacLeod
N."The
7
Benefits
of
Self-Directed
Learning"
Published
on
August
11,
2015
https://www.linkedin.com/pulse/7-benefits-self-directed-learning-nancy-macleod.
13)
Harden,
R.
M.
A
new
vision
for
distance
learning
and
continuing
medical
education.
Journal
of
Continuing
Education
in
the
Health
Professions
.2005;25:
43-51
14)
Wood
Diana
F.
ABC
of
learning
and
teaching
in
medicine:
Problem
based
learning.
BMJ
2003;326:328-330.
15)
Miflin
BM,
Campbell
CB,
Price
DA.
A
conceptual
framework
to
guide
the
development
of
self-directed,
lifelong
learning
in
problem-based
medical
curricula.
Med
Educ.2000;34:299-306.
16)
Brockett
R
G
and
Hiemstra
R
.
Self-Direction
in
Adult
Learning:
Perspectives
on
Theory,
Research,
and
Practice.
London
and
New
York:
Routledge;
1991.
Available
on
the
internet;
http://home.twcny.rr.com/hiemstra/sdlindex.html.
17)
Guglielmino,
L.M.
The
case
of
promoting
self-directed
learning
in
formal
educational
institutions.
SA-eDUC
JOURNAL
2013;(10):
2.
18)
Lunyk-Child,
O.,
Crooks
D.,
Ellis
P.,
Ofosu
C.,
O´Mara
L.,
Rideout
E.
"Self-directed
learning:
faculty
and
student
perceptions",
J
Nurs
Edu.
2001;40(3
):
116-123.
19)
Van
Schaik
S,
Plant
J,
and
O'Sullivan
P.
Promoting
self-directed
learning
through
portfolios
in
undergraduate
medical
education:
The
mentors'
perspective.?2012;Medical
Teacher,
35(2).
20)
Ali
PA,
Panther
W
.
Professional
development
and
the
role
of
mentorship.
Nurs
Standard.2008
;22(42):
35-39.
21)
Dolmans
HJM,
Schmidt
HG
.
What
drives
the
student
in
problem-based
learning?
Med
Educ.1994;28:372-80.
22)
Bamidis
P
.
The
Effectiveness
of
Blended
Learning
in
Health
Professions:
Systematic
Review
and
Meta-Analysis.
J
Med
Internet
Res
.2016;
18(1):
e2.
23)
Den
Harder
A
,
Frijlingh
M,
Ravesloot
C,
Oosterbaan
AE,
and
van
der
Gijp
A.
The
Importance
of
Human-Computer
Interaction
in
Radiology
E-learning
.
J
Digit
Imaging.
2016;
29(2):
195-205.
24)
Moin
M,
Sadia
S,
Naqi
S.
STUDENT
PERSPECTIVE
ABOUT
ONE
MINUTE
PRECEPTORSHIP
IN
A
BUSY
OUTPATIENT
SETTING
.
Pak
Armed
Forces
Med
J.
2016;
66
(1):162-66
25)
Robles
J.
Student
Learning
Contracts:
Considerations
for
Implementation
in
Pharmacy
Experiential
Experiences.
J
Pharma
Care
Health
Sys
.2015;2:
135.
doi:10.4172/2376-0419.1000135
26)
Amandu
GM,
Muliira
JK,
Fronda
DC.
Using
moodle
e-learning
platform
to
foster
student
self-directed
learning:
Experiences
with
utilization
of
the
software
in
undergraduate
nursing
courses
in
a
Middle
Eastern
university
.
Procedia
-
Social
and
Behavioral
Sciences.
2013;
(93):
677
-
683.
27)
Challis
M
.AMEE
medical
education
guide
no.
11
(revised):
Portfolio-based
learning
and
assessment
in
medical
education.
Med
Teach.
1999;
21:
370-86.
28)
Toolbox
of
Assessment
Methods,
Version
1.1.
Accreditation
Council
for
Graduate
Medical
Education
(ACGME),
&
American
Board
of
Medical
Specialties
(ABMS).2000;
Available
online:
http://www.acgme.org/Outcome/assess/Toolbox.pdf
29)
Dent,
J.A.,
Harden,
R.M.
A
practical
guide
for
medical
teachers.
Elsevier,
Second
Edition,
chapters
7
and
16.
2005.
30)
Cunningham
D,
McCalister
P
and
MacVicar
R
.
Practice-based
small
group
learning:
what
are
the
motivations
to
become
and
continue
as
a
facilitator?
A
qualitative
study
.
Quality
in
Primary
Care.
2011;19:5-12
31)
Mazmanian
P.
and
Feldman
M.
Theory
is
needed
to
improve
education,
assessment
and
policy
in
self-directed
learning.
Medical
education.
2011;45(4),
324-6.
32)
Carr
L
.
Seven
Preceptor
Microskills:
Pearls
for
More
Effective
&
Efficient
Clinical
Teaching.
Published
on
November
26,
2015
https://www.linkedin.com/pulse/7-preceptor-microskills-pearls-more-effective-linda-carr-ph-d-?trk=mp-reader-card
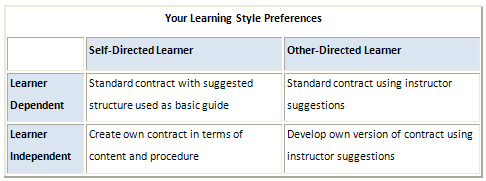
A.
LEARNING
CONTRACTS
In
developing
your
learning
contract,
it
may
be
useful
if
you
have
a
sense
of
your
own
learning
and
cognitive
styles.
The
following
figure
is
provided
to
facilitate
the
learner
who
has
never
filled
out
a
learning
contract
in
obtaining
some
sense
of
what
might
be
the
best
approach
for
this
course.
 SOME
GUIDELINES
FOR
THE
USE
OF
LEARNING
CONTRACTS
SOME
GUIDELINES
FOR
THE
USE
OF
LEARNING
CONTRACTS
(Murad
MH,
2008).
How
do
you
develop
a
learning
contract?
Step
1:
Diagnose
your
learning
needs.
Step
2:
Specify
your
learning
objectives.
Step
3:
Specify
learning
resources
and
strategies.
Step
4:
Specify
target
dates
for
completion.
Step
5:
Specify
evidence
of
accomplishment.
Step
6:
Specify
how
the
evidence
will
be
validated.
Step
7:
Review
your
contract
with
consultants.
Step
8:
Carry
out
the
contract.
Step
9:
Evaluation
of
your
learning.
B.
Types
of
Tools
and
resources
used
in
SDL
((Murad
MH,
2008).
|

