|
Bader A. Almustafa,
MBBS, DPHC (RCGP), ABFM, SBFM
Consultant Family Physician
Hypertension and CVR clinic
Qatif Primary Health Care
P.O. Box 545, Qatif 31911,
Saudi Arabia
Tel: +966 3 852 6834,
Fax: +966 3 852 2711,
E-mail: bader@alqtif.org
|
During
the last decade many guidelines have been
published for detection, evaluation and
treatment of different cardiovascular disease
(CVD) risk factors (RF) including hypertension
(HTN), diabetes mellitus (DM), dyslipidemia,
and obesity. Many of these were evidence-based,
vigorously reviewed and regularly updated.
Nevertheless,
guidelines were not sufficient to change
neither the outcome nor the behavior of
caregivers. Several studies have shown that
clinicians often fail to collect, routinely,
even basic information such as plasma lipids,
blood pressure (BP) and cigarette smoking
status during the course of medical care.[17,18]
This failure
has been explained by many barriers, identified
earlier. Among these are the lack of knowledge
and poor communication skills of the practicing
physicians, lack of self efficacy, oversight,
discontinuity of care, lack of communication
between providers caring for the same patient,
lack of external barriers, lack of auditing,
pressure of work, co-morbid illness, along
with the diverse and complex work-up needed
for chronic problems at different stages
of their progress.[17,18,20,22] Practicing
physicians may find this work-up time-consuming,
[23] as most of the consultation time is
spent in looking-up different pages in the
medical chart, which might belong to previous
visits in the last few months or even years,
in order to find, compare and interpret
laboratory results and blood pressure readings.
Another
difficulty that may add to the burden is
the need to reduce the risk for CVD which
includes the recall of all necessary details
needed for:[23]
- the identification
and measurement of RF and collection
of clinical data relevant for assessing
these factors;
- the interpretation
of risk-related data with estimation
of total CVD risk, which is highly missed;
- and the use of
therapeutic intervention to minimize
CVD risk or to prevent the development
of additional RF.
The principle of assessing
total risk associated with multiple CVD
risk factors has been well stated since
its first introduction in New Zealand
in 1993, and followed thereafter, by many
guidelines, worldwide. It provides more
logical approach to patient management,
as it approaches the whole patient and
every aspect of his risk to develop CVD.
It predicts short-term benefits and provides
accurate data to substantiate a physician's
clinical judgment. This is particularly
true by identifying those individuals
who, while asymptomatic, will potentially
benefit from risk-reducing interventions.[26]
This article describes
4 pages of evidence-based encounter forms
(EF) that have been developed by the author
to facilitate office assessment, follow-up
and audit of services delivered to patients
with chronic CVD risk factors. They are
used in the initial clinical assessment
of patients presenting with high readings
of BP, fasting blood sugar (FBS), total
cholesterol or body mass index (BMI).
In addition, they provide a tool for stratification
of CVD risk, regular follow up and annual
assessment.
The development of
these forms started in the late 1990's.
At that time, many constraints were noticed
by the author regardingthe use of the
locally available forms assigned, at that
time, for the follow up of either hypertension
or diabetes. Although, they had a significant
advantage in auditing the work, they lacked
convenience in office use. Their application
involves extra work and time. Physicians
need to go through many papers and forms
to browse and fill. On the other hand,
they do not offer any guide for initial
assessment and do not consider all risk
factors in one view.
On this background,
the author started to look for the practice
of other institutions, during his visits
to different regions and countries, in
addition to browsing for the internationally
published ones. Unfortunately, none of
these have been considered for use in
neither initial CVD risk assessment nor
the estimation of this risk. They were,
merely, used in the follow up of either
hypertensive or diabetic patients, which
included ,their best, blood pressure readings,
blood sugar, urine dipstick results, and/or
medications.
The presently described
EF have considered, in their design, the
constraints and needs presented above,
to be evidence-based and the need to have
a total CVD risk assessment approach.
For these reasons,
current local and international guidelines
that consider detection, evaluation or
management of CVD risk factors were reviewed
and their recommendations were put in
view.
EF, then, were put
in practice and were periodically reviewed
to meet up-to-date recommendations and
goals of their development. The latest
version was reviewed upon current guidelines,
protocols, and references shown below,
in addition to comments collected from
practicing physicians and nurses.[1,2,3,4,5,6,7,8,9,10,11,29,33,39,41,43,44,45]
|
|
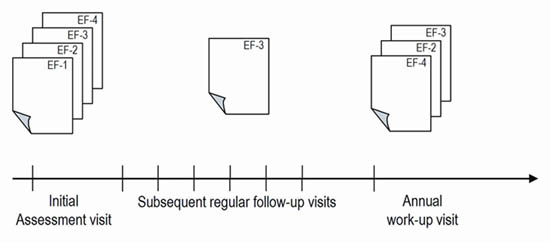
Figure 1 shows the temporal
use of the described EF. The initial assessment
visit needs the use of all four forms, while
the regular follow-up visit necessitates
the use of one form only. However, the annual
assessment requires three of them to be
used.
EF-1 (Figure 2) is the
initial-visit assessment form. It is intended
for use in the initial assessment of newly
attending patients with CVD risk factors,
mentioned above. It contains eight sections
for demographic data, history taking, physical
examination and investigations. It assists
in identifying confounding RF, target organ
damages (TOD), associated clinical conditions
(ACC) and secondary causes such as renal,
vascular and endocrine diseases. In addition,
a table has been included to help in staging
the BP level.
EF-2 (Figure 3) is the
CVD risk stratification form. It is tailored
to supplement both EF-1 and EF-4. It helps
summarize and stratify CVD risk. The risk
assessment tool, presented in the European
guidelines for management of hypertension,
was used for this purpose.3 Two tables are
provided in this EF; the first table provides
a check list of RF, TOD and ACC collected,
earlier, using EF-2 or EF-4. This list makes
stratification of total CVD risk easier,
using the second table. EF-2 might be filled
in by the physician or the attending nurse.
On the other hand, EF-2
provides a chance to compare the progress
in total CVD risk among the years of follow-up.
EF-3 (Figure 4) is the
regular follow-up flow chart. It is used
in each visit the patient pays to the clinic.
It contains four sections and 14 columns.
Each column is intended for use in one visit.
One section has reserved spaced for more
frequently monitored parameters, i.e. vital
signs, urinary dipstick and blood chemistry.
These help in monitoring the control and
early detection of hemodynamic - and biochemical
drug adverse effects. The uppermost section
is allocated for plotting blood pressure
readings. It allows for quick evaluation
of control of BP over the last few visits.
Documentation of medication refills and
changes in dose requirement are possible
for six medications, each in one line.
Patient's compliance
is readily reviewed and documented using
a mnemonics (DEMO) created for this purpose,
where D, E, M and O stand for diet, exercise,
medication and others (such as smoking,
hygiene and foot care), respectively. In
the same pattern health education is reviewed
and documented. DEMO functions as a reminder
for the physician to inquire about patient's
compliance and to provide appropriate education.
Advantages of the
use of CVR Encounter Forms.
- Facilitate and empower
initial assessment and follow-up of different
CVD risk factors in one common form.
- Simplify stratification
of CVD risk, and thus approaching patients
more appropriately.
- Minimize the time
needed in assessment and follow-up.
- Enable physicians
to compare the status of current visit
with previous visits and identify defect
in service and control, easily. The comparison
can be used as reflection that can be
shown to patients to help them improving
their compliance.
- Function as a reminder
for care. They prompt care giver to address
this issue during every visit, even if
the patient is presenting for unrelated
complaint, such as cut wounds.
- Improve quality of
service, documentation and ensure uniform
data entry.
- Facilitate communication
between providers caring for the same
patient.
- Facilitate the audit
work in readily structured process.
Decision of referral
to other services such as nephrology, dietary,
ophthalmology, or echocardiography can be
documented in an exclusive field in the
lower part of the form. At the bottom, two
fields were allocated for extra notes, such
as reason to change regimen, and expected
next visit.
The last form EF-4 (Figure
5) is the annual assessment chart. It acts
as a reminder for the annual work-up needed
for CVD risk patients and provides, in addition,
a tool to compare progress in control of
risk, development of TOD and complications,
as well as hemodynamic and biochemical changes
secondary to medications used. Parameters
needed for estimation of CVD risk are labeled
by a super text. Additionally this form
is used, by the auditors to evaluate process
and outcome achieved.
Many advantages have
been noticed by the author from the use
of EF-1 through to EF-4 (box 1). However,
the extra use of such forms necessitated
regular update and regular orientation for
newly employed staff, which were, thankfully,
encouraging for the development of the forms.
In conclusion, caring for
patients with multiple CVD risks is a demanding
task that physicians usually fail to fulfill,
as per guidelines. This article describes
the development of evidence-based encounter
forms that help physicians and nurses to
put guidelines into practice. Validation
of these forms on a wider scale is needed
to show their significance.
The author would like to thank
all physicians and nurses who have relayed
their comments and suggestions on the content
and design of the forms. Particular thanks
to Rania Al-Mousa, RN, Dr. Fatima Al-Dubaisi
and Dr. Mohammed Al-Zaher for their valuable
comments. Thanks are extended to my sincere
students Zainab Al-Duhaileb and Jumana Al-Jishi
for their editing support. Special appreciation
for my wife Azhar Al-Juma and my daughter
Fatima for their valuable design support.
|
| 1. |
Chobanion AV, Bakris GL,
Black HR, Cushman WC, Green LA, Izzo
JL, et al. The seventh report of the
Joint National Committee on Prevention,
Detection, Evaluation, and Treatment
of High Blood Pressure: The JNC 7 Report.
JAMA. 2003;289:2560-2572. |
| 2. |
World Health Organization,
International Society of Hypertension
Writing Group. 2003 World Health Organization
(WHO)/International Society of Hypertension
(ISH) statement on management of hypertension.
Journal of Hypertension 2003, 21(11):1983-1992. |
| 3. |
Guidelines Committee.
2003 European Society of Hypertension-European
Society of Cardiology guidelines for
the management of arterial hypertension.
Journal of Hypertension 2003, 21:1011-1053. |
| 4. |
Williams B, Poulter NR,
Brown MJ, Davis M, McInnes GT, Potter
JF, et al. Guidelines for management
of hypertension: report of the fourth
working party of the British Hypertension
Society, 2004-BHS IV. J Hum Hypertens
2004;18: 139-85. |
| 5. |
Canadian Hypertension
Education Program. Khan NA, McAlister
FA, Campbell NR, Feldman RD, Rabkin
S, Mahon J, Lewanczuk R, Zarnke KB,
Hemmelgarn B, Lebel M, Levine M, Herbert
C. The 2004 Canadian recommendations
for the management of hypertension:
Part II--Therapy. Can J Cardiol. 2004
Jan;20(1):41-54. |
| 6. |
Working Party of the International
Diabetes Federation (European Region).
Hypertension in people with Type 2 diabetes:
knowledge-based diabetes-specific guidelines.
Diabet Med. 2003 Dec;20(12):972-87. |
| 7. |
National Task Force on
the Prevention and Treatment of Obesity.
Medical care for obese patients: advice
for health care professionals. Am Fam
Physician 2002;65:81-8. |
| 8. |
Expert Panel on Detection,
Evaluation, and Treatment of High Blood
Cholesterol in Adults. Executive Summary
of the Third Report of the National
Cholesterol Education Program (NCEP)
Adult Treatment Panel III. Bethesda,
Md.: National Institutes of Health;
2001. NIH Publication No. 01-3670. |
| 9. |
Expert Panel on the Identification,
Evaluation, and Treatment of Overweight
and Obesity in Adults. Clinical guidelines
on the identification, evaluation, and
treatment of overweight and obesity
in adults: evidence report. Bethesda,
Md.: National Heart, Lung, and Blood
Institute Obesity Education Initiative;
1998. NIH Publication No. 98-4083. |
| 10. |
Scottish Intercollegiate
Guidelines Network. Management of Diabetes.
A national clinical guideline. November
2001. 50 pages. |
| 11. |
British Cardiac Society,
British Hyperlipidaemia Association,
British Hypertension Society, British
Diabetic Association. Joint British
recommendations on prevention of coronary
heart disease in clinical practice:
summary. BMJ 2000;320:705-6. |
| 12. |
Kottke TE, Solberg LI,
Brekke ML, Cabrera A, Marquez MA. Delivery
rates for preventive services in 44
midwestern clinics. Mayo Clin Proc.
1997 Jun;72(6):515-23. |
| 13. |
Cuspidi C, Michev I, Lonati
L, Vaccarella A, Cristofari M, Garavelli
G, et al. Compliance to hypertension
guidelines in clinical practice: a multicentre
pilot study in Italy. J Hum Hypertens.
2002 Oct;16(10):699-703. |
| 14. |
M Akel and
G Hamadeh. Quality of diabetes care
in a university health center in Lebanon.
Int J Qual Health Care 1999 11: 517-521.
|
| 15. |
Al-Mustafa
BA, Abulrahi HA. The role of primary
health care centers in managing hypertension.
How far are they involved? Saudi Med
J. 2003 May;24(5):460-5. |
| 16. |
Putzer G,
Roetzheim R, Ramirez AM, Sneed K, Brownlee
HJ Jr, Campbell RJ. Compliance with
recommendations for lipid management
among patients with type 2 diabetes
in an academic family practice. J Am
Board Fam Pract. 2004 Mar-Apr;17(2):101-7. |
| 17. |
Mottur-Pilson
C, Snow V, Bartlett K. Physician explanations
for failing to comply with "best practices".
Eff Clin Pract. 2001 Sep-Oct;4(5):207-13.
|
| 18. |
Cabana MD,
Rand CS, Powe NR, Wu AW, Wilson MH,
Abboud PA, Rubin HR. Why don't physicians
follow clinical practice guidelines?
A framework for improvement. JAMA. 1999
Oct 20;282(15):1458-65. |
| 19. |
Hobbs FD.
Cardiovascular risk management in primary
care. Diabetes Obes Metab. 2002 Nov;4(6):362-7
|
| 20. |
van Steenkiste
B, van der Weijden T, Stoffers HE, Grol
R. Barriers to implementing cardiovascular
risk tables in routine general practice.
Scand J Prim Health Care. 2004 Mar;22(1):32-7.
|
| 21. |
Javors JR,
Bramble JE. Uncontrolled chronic disease:
patient non-compliance or clinical mismanagement?
Dis Manag. 2003 Fall;6(3):169-78. |
|
|
| 22. |
Maue SK,
Segal R, Kimberlin CL, Lipowski EE.
Predicting physician guideline compliance:
an assessment of motivators and perceived
barriers. Am J Manag Care. 2004;10(6):383-91. |
| 23 |
Ketola E,
Sipila R, Makela M, Klockars M. Quality
improvement programme for cardiovascular
disease risk factor recording in primary
care. Qual Health Care. 2000 Sep;9(3):175-80.
|
| 24. |
Philip Greenland, Scott
Grundy, Richard C. Pasternak, Claude
Lenfant. Problems on the Pathway From
Risk Assessment to Risk Reduction. Circulation
1998;97:1761-1762. |
| 25. |
Jackson R, Barham P, Bills
J, Birch T, McLennan L, MacMahon S,
Maling T. Management of raised blood
pressure in New Zealand: a discussion
document. BMJ. 1993;307:107-10. |
| 26. |
Sidney C. Smith, Jr, Rod
Jackson, Thomas A. Pearson, Valentin
Fuster, Salim Yusuf, Ole Faergeman,
et al. Principles for National and Regional
Guidelines on Cardiovascular Disease
Prevention: A Scientific Statement From
the World Heart and Stroke Forum. Circulation
2004 109: 3112 - 3121. |
| 27. |
Susanna E. Guzman. Practical
Advice for Family Physicians to Help
Overweight Patients. American Academy
of Family Physicians; 2003. |
| 28. |
Qatif Primary Health Care.
Hypertension and diabetes mellitus encounter
forms. Qatif (Saudi Arabia): Ministry
of Health; 1997. |
| 29. |
Qatif Primary Health Care.
Chronic Disease Nursing Protocol. Qatif
(KSA): Ministry of Health; 2001. |
| 30. |
Khobar Primary Health
Care. Hypertension and diabetes mellitus
encounter forms. Khobar (Saudi Arabia):
Ministry of Health; 1997. |
| 31. |
King Fahad Hospital of
the University. Diabetes mellitus encounter
forms. Khobar (Saudi Arabia). King Fahad
University; 1990. |
| 32. |
King Abdulaziz University
Hospital. Diabetes mellitus encounter
forms. Riyadh (Saudi Arabia). King Saud
University; 1994. |
| 33. |
Khoja T. Chronic diseases
guideline in primary care. Ministry
of health. 1st edition; Apr 2001. 80
pages, p 40-50. |
| 34. |
Al-Mazrou YY, Farag MK.
The Scientific Committee of Quality
Assurance in Primary Health Care. Quality
Assurance in Primary Health Care Manual.
1st ed. Riyadh (KSA): WHO-EM/PHC/81-A/G/93.
1994. p. 145-146. |
| 35. |
O'Brien E, Beevers D.G.,
Marshall H., ABC hypertension. BMJ publishing
group. 3rd edition; July 1995; 92 pages.
|
| 36. |
1999 World Health Organization-International
Society of Hypertension Guidelines for
the Management of Hypertension. Journal
of Hypertension 1999, 17:151-183 |
| 37. |
Joint National
Committee on Detection, Evaluation,
and Treatment of High Blood Pressure.
The sixth report of the Joint National
Committee on Prevention, Detection,
and Treatment of High Blood Pressure
(JNC VI). Arch Intern Med 1997;157:2413-2446. |
| 38. |
Lawrence
E Ramsay, Bryan Williams, G Dennis Johnston,
Graham A MacGregor, Lucilla Poston,
John F Potter, Neil R Poulter, Gavin
Russell. British Hypertension Society
guidelines for hypertension management
1999: summary. BMJ 1999;319:630-5. |
| 39. |
Wood D,
Durrington P, Poulter N, et al. Joint
British recommendations on prevention
of coronary heart disease in clinical
practice. Heart 1998;80(suppl 2):S1-29.
|
| 40. |
Qatif Primary
Health Care. Chronic Disease Nursing
Protocol. Qatif (KSA): Ministry of Health;
1996. |
| 41. |
American
Diabetes Association. Standards of medical
care for patients with diabetes mellitus.
Diabetes Care 2003;26(Suppl 1):S33-50.
|
| 42. |
Mulrow CD.
Evidence-based Hypertension. BMJ publishing
group. 1st edition; 2001. |
| 43. |
Beevers G,
Lip GY, O'Brien E. ABC of hypertension.
BMJ publishing group. 4th edition 05/2001.
page 96 |
| 44. |
Ebell MH.
A Tool for Evaluating Hypertension.
Family Practice Management. March 2004:79-81.
|
| 45. |
C. Carolyn
Thiedke. From Page to Practice: Improving
Care of Type 2 Diabetes. American Academy
of Family Physicians; 2004. |
| 46. |
Poulter NR.
Benefits and pitfalls of cardiovascular
risk assessment. J Hum Hypertens. 2000.
|
|