|
Storage of Medicines
and Temperature Control at Community Pharmacies
in Rural District of Sindh, Pakistan: An Exploratory
Cross-Sectional Study
Nadir Suhail
(1)
Sumera Aziz Ali (2)
Waris Qidwai (3)
Savera Aziz Ali (4)
Saleem Iqbal (2)
Yousaf Memon (2)
Mohammad Masood Kadir(2)
(1) Monitoring and Evaluation consultant deliver
project USAID, Pakistan
(2) Department of Community Health Sciences
Aga Khan University, Karachi Pakistan
(3) Department of Family medicine Aga Khan University,
Karachi Pakistan
(4) School of Nursing Aga Khan University, Karachi
Pakistan
Correspondence:
Dr. Waris Qidwai
Professor and Chairman,
Family Medicine Department
Aga Khan University Karachi Pakistan
Tel: (92-21) 486-4843, 486-4814
Fax: (92-21) 493-4294, 493-2095
Email: waris.qidwai@aku.edu
|
Abstract
Background: Medicines
are the essential tools for prevention,
cure and control of diseases. If these
medicines are ineffective then their aftermath
can cause wastage of resources. Medicines
lose their required effectiveness due
to inadequate storage at required temperature.
Objective: The
objective was to estimate the proportion
of pharmacies with high temperature (>25°C)
inside pharmacy outlets in two talukas
(sub-districts) of district Thatta, Sindh
Methodology:
An exploratory cross sectional study
design was conducted from August 2013
to August 2014. All pharmacies of the
two talukas were approached by doing a
census. Descriptive analysis was done
to calculate the frequencies and proportions.
Results: All pharmacies (n=62)
had a temperature of >25?C inside the
pharmacies. Medicines were exposed to
sunlight in 39 (63%) of the pharmacies
and 39 (63%) of pharmacies had refrigerators
to keep insulin and vaccines. Median duration
of electricity shut downs was 12 hours
per day and 11% of the pharmacies had
back up power supply.
Conclusion: More than a quarter
of pharmacy owners were aware about maintaining
the required temperature of < 25?C
but none of them were maintaining required
temperature. Considering the electricity
shut down, it is important to make cost
effective and long term strategies to
maintain the efficacy of medicines. Proper
legislation needs to be enforced with
continuing training programs for pharmacy
owners. Further research is required to
explore different ways of maintaining
required temperature to ensure the adequate
efficacy of medicines.
Key words:
Pharmacy, Temperature control, Storage,
Medicines
|
Medicines including vaccines are considered
as one of the important tools in combating diseases
across the world, but these medicines may also
cause adverse events with varying severity which
usually depend upon patient as well as product
related factors(1). This issue is even more
critical in developing countries where most
medications are not stored at appropriate conditions
and can be easily purchased over the counter(1).
Medicinal products require appropriate storage
conditions in order to ensure the quality and
efficacy of medicines (2). Medicines which are
not stored on required temperature (< 25?
C) can further increase unnecessary burden on
economy of general population due to their ineffectiveness
in curing of disease (2).
Literature shows that stability of pharmaceutical
products is extremely essential to maintain
their therapeutic efficacy(3). Temperature plays
a key role to maintain the required efficacy
of medicines (4-6). It has been suggested that
more than 50% of medicines should be stored
on required temperature, which is usually less
than 25?C (6-8). Apart from high temperature
(> 25°C), direct exposure to sunlight
and improper management of medicines during
shipment can also cause damage to pharmaceutical
products like antivirals, multi-vitamins, acetaminophens,
antibiotics, diuretics, hydrocortisone, eye
drops, analgesics, anti-depressants and latex
products such as male condoms (9, 10). Light
can change the properties of different materials
and products. This change in properties can
be due to steadily increasing exposure of medicines
to high temperature during storage or dispensing
the medicines at the pharmacies through different
mechanisms(11, 12).
Almost every country in the world has some
mechanism of providing drugs to people residing
in communities, either through proper prescription
or without prescription of medications. These
countries have retail and wholesale pharmacies
working regularly to serve their community (1).
likewise other countries, there are an estimated
45 000 to 50 000 wholesale and retail drug outlets
in Pakistan (1). Although there is a network
of health services in Pakistan's public sector,
and overabundance of private sector initiatives,
45% of the population still lacks access to
health services (13). Thus, in order to meet
health needs and to reduce out of pocket payment,
people rely on alternative health care systems
such as traditional medicine practitioners,
chemists, faith healers, and homeopaths(1).
Self-medication has been consistently increasing
due to large gaps in the formal health sector
of the country (1).
Furthermore, people usually rely on the nearby
accessible medical stores or small community
pharmacies to purchase medicines for different
diseases (14, 15). In many countries, community
pharmacies are places where people may obtain
health advice and assistance to manage their
disease states with required medications (16).
Moreover, these pharmacies are often the first
point of contact for patients seeking health
care as they are usually more accessible and
less socially distant than other providers including
medical doctors (1). Community pharmacies have
been considered as a key interface between the
health care system and the general public (14,
15). It is common that many workers at community
pharmacies are involved in providing health
advice on most of the health problems prevailing
in community (14, 15). Even most of the times,
community pharmacy workers prescribe medicines,
which are sometimes safe and effective when
used correctly, however these can become dangerous
in case of emergencies (17, 18). Community pharmacies
are perceived as an easy and convenient source
of advice, referral to nearby facility and source
of required information by the patients and
their families in developing world, including
Pakistan (19, 20).
Community pharmacy owners can be considered
as one of the important influential stakeholders
in health care system who can affect the drug
usage owing to their scale of operations and
placement in the healthcare delivery system
(21). Looking at importance of community pharmacies
and their outreach services, many developing
countries have used their potential to promote
safe and effective treatments (17). This has
been done by enhancing their dispensing practices
and management of medicines inside pharmacy
outlets and in stores, which are easily acceptable
to community pharmacy workers and their owners
(17).
In Pakistan unfortunately the area of community
pharmacy has been ignored by policymakers to
make collaboration of community pharmacy workers
and owners with other stake holders in health
sector of country for the betterment of population.
Therefore it is essential to work in team by
including community pharmacy workers for betterment
of general population (22)
Thus it is essential to know the importance
of community pharmacies in the context of temperature
management during hot weather and particularly
in rural areas of Pakistan (23).
Click here for
Figure 1: Storage Practices in retail Pharmacies
at District Level: A conceptual Framework
Furthermore, in Pakistan there is an issue of
increased electricity shut downs in rural areas
even for more than 12 hours which prevents storing
medicines at required temperature in community
pharmacies of rural areas of Pakistan. Community
pharmacies are one of the important sources
of dispensing medicines to the Pakistani population.
Knowledge about proper storage of medicines
at required temperature in community pharmacies
is not available. In country like Pakistan many
other issues also arise in hot weather and it
is a challenge to store the medicines appropriately
on required temperature due to electricity shut
downs and lack of backup power supply (23).
Thus, it is important to know that whether the
medicines are stored on required temperature
or not, particularly in community pharmacies
of rural areas.
This study had assessed the practices regarding
storage of medicines in rural area of Sindh,
Pakistan. This study was aimed to estimate the
proportion of pharmacies with high temperature
(> 25 °C) inside the pharmacy outlets
in Sindh Pakistan and to estimate the proportion
of pharmacies selling vaccines, insulin and
have refrigerators with and without backup power
supply. This information will contribute to
improve policies for managing and storing medicines
appropriately especially in remote areas of
Sindh.
Exploratory cross sectional study design was
used to conduct this study form August 2013
to August 2014. This study was conducted in
two areas of the Thatta district. These areas
included two talukas (sub-districts), Sujawal
and Jati. Thatta is a rural district in the
southernmost part of Sindh province in Pakistan,
bordering Karachi (24). The estimated population
of district is around 1513194 (25) with literacy
rate of 22.1% (26). There are five public sector
hospitals in Thatta, as well as 8 rural health
centers (RHCs) and 51 basic health units (BHUs).
Those community pharmacies which were selling
at least allopathic medicines in the two talukas
(sub-districts) of district Thatta (Sujawal
and Jati) and whose pharmacy owners gave the
written informed consent were included in this
study. While those pharmacies, which were located
in the hospital premises or where a medical
doctor was practicing were excluded from this
study.
We did a census for all pharmacies of two talukas
(sub-districts) to get the list of eligible
pharmacies. The census covered a total of 70
pharmacies and all 70 pharmacies and their pharmacy
owners or drug sellers were approached but 8
pharmacies refused to give the informed consent
thus could not be included in the study. Thus
62 pharmacies were included through consecutive
non-probability sampling.
Pharmacy owners were interviewed through a structured
and pretested questionnaire. A checklist was
also used to assess the storage conditions in
the community pharmacies during month of June
and July 2014. Room thermometer was used to
measure the temperature in all the selected
pharmacies. Three digital thermometers and three
mercury maximum/minimum thermometers were purchased
and checked by comparing these thermometers
with standard thermometer in biomedical department
of Aga Khan University for 20 hours. The biomedical
department engineers agreed within standard
deviation of 0.2°C. Two digital thermometers
along with mercury thermometers were placed
in every community pharmacy for half an hour.
One thermometer was kept in outer half of the
community pharmacy where first drug was placed
and one in inner half of the community pharmacy
along where last drug was placed. Over the same
period of time maximum ambient air temperature
of Karachi was also noted from website of Pakistan
meteorological department, whose results displayed
on different web pages. Three readings of the
temperature were taken at three different timings
of the day. The maximum temperature in the day
was recorded at 1500 hours of each day. After
taking the three readings, an average value
of all readings was taken to overcome the intra
rater bias.
Data was analyzed through SPSS version 19. Frequencies
and proportions were generated for all the variables.
Estimated prevalence of pharmacies with high
temperature (>25 °C) was calculated.
Descriptive statistics were computed for both
continuous and categorical variables. This study
was conducted only after ethical approval by
Ethical Review Committee (ERC) of the Aga Khan
University.
From
a
total
of
70
pharmacies,
62
pharmacy
owners
expressed
their
willingness
to
participate
in
the
study,
making
the
interview
response
rate
as
95%.
Median
duration
of
service
provision
by
pharmacy
owners
in
the
community
was
8
years
with
interquartile
range
(IQR)
of
6-10
years
(Table
1).
Table
1:
Knowledge
of
pharmacy
owners
about
temperature
and
storage
practices
(n=62)
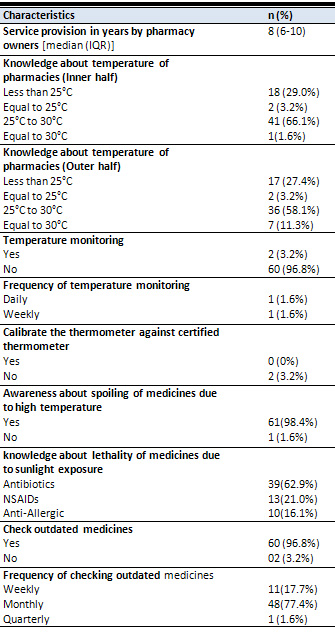
With
respect
to
knowledge
about
temperature
of
pharmacies,
18
(29%)
of
the
pharmacy
owners
reported
that
temperature
of
inner
half
of
pharmacy
should
be
below
25
°C,
41
(66%)
reported
that
temperature
of
inner
half
of
pharmacy
should
be
between
25
°C
and
30
°C,
2
(3%)
pharmacy
owners
reported
that
temperature
should
be
equal
to
25°C,
and
1
(2%)
reported
that
temperature
should
be
equal
to
30°C.
With
respect
to
the
temperature
of
outer
half
of
pharmacy,
17
(27%)
of
the
pharmacy
owners
reported
that
temperature
should
be
less
than
25°C,
36
(58%)
pharmacy
owners
said
that
it
should
be
between
25°C
and
30°C,
7
(11%)
owners
reported
that
temperature
should
be
equal
to
30°C,
while
2
(3%)
pharmacy
owners
reported
that
temperature
should
be
equal
to
25°C.
Regarding
temperature
monitoring,
2
(3%)
pharmacy
owners
reported
that
they
used
to
monitor
the
temperature
of
main
pharmacy
with
a
room
thermometer
but
none
of
them
used
to
maintain
the
temperature
of
storage
area
up
to
required
level.
Out
of
these
2
pharmacies,
1
(2%)
pharmacy
owner
reported
to
monitor
the
temperature
on
a
daily
basis
while
1(2%)
reported
to
monitor
the
temperature
on
a
weekly
basis.
None
of
them
used
to
calibrate
the
thermometer
against
the
certified
thermometer
(Table
1).
Regarding
the
knowledge
about
toxic
effects
of
medicines
due
to
sunlight
exposure,
39
(63%)
of
the
pharmacy
owners
reported
that
antibiotics
can
become
ineffective
if
exposed
to
sunlight,
followed
by
13
(21%)
owners
indicating
NSAIDS
become
ineffective
upon
sunlight
exposure
(Table
1).
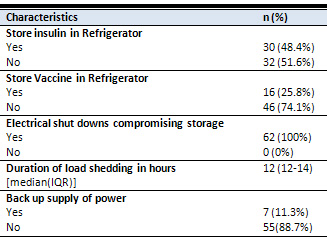
Out
of
62
pharmacies,
30
(48%)
pharmacy
owners
reported
selling
of
insulin;
all
of
them
used
to
keep
the
insulin
in
refrigerators.
Sixteen
(26%)
pharmacy
owners
reported
selling
of
vaccines
and
keeping
them
in
refrigerators.
Regarding
electricity
shut
down,
all
owners
reported
that
they
face
this
problem
in
their
respective
talukas;
its
median
duration
being
12
hours
per
day
(IQR:
12-14hrs)
but
only
7
(11%)
pharmacies
had
a
backup
supply
of
power
(Table
2).
Table
2:
Storage
practices
of
the
medicines
required
to
be
stored
in
cool
place
(n=62)
Furthermore,
35
(56%)
pharmacies
were
found
to
have
items,
grouped
in
amounts
that
are
easy
to
count.
With
respect
to
expired
medicines,
all
62
pharmacy
owners
used
to
keep
the
items
with
short
expiry
dates
in
front,
while
those
medicines
which
had
long
expiry
date
were
placed
at
the
back
("first
expired
first
out"
principle).
9
(15%)
pharmacies
were
maintaining
the
record
for
the
removal
of
items
including
date,
time,
witness
and
manner
of
removal
(Table
3).
Table
3:
Findings
regarding
storage
of
medicines
in
main
pharmacy
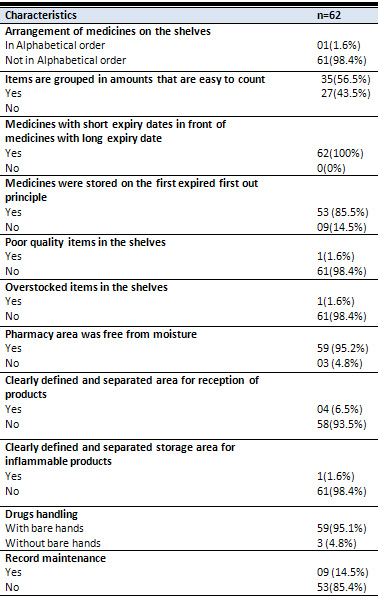
Approximately
1.6%
of
the
pharmacies
were
found
to
have
the
poor
quality
items
in
the
shelves
and
similar
proportion
had
any
overstocked
items
in
the
shelves
(Table
3).
Moreover,
the
floors,
walls,
sinks,
benches,
shelves,
containers
and
dispensing
bottles
were
found
to
be
clean
in
about
59
(95%)
pharmacies.
Only
4
(6%)
pharmacies
had
a
clearly
defined
area
for
reception
of
products,
and
3
(5%)
pharmacy
owners
reported
that
drugs
are
not
handled
with
bare
hands
(Table
3).
All
of
the
62
pharmacies
(100%)
had
a
temperature
of
>25°C
(Table
4).
In
39
(63%)
pharmacies,
sunlight
exposure
to
medicines
was
evident.
Among
the
medicines
exposed
to
sunlight,
NSAIDs
comprised
the
major
proportion
(51.2%),
followed
by
antibiotics
(38.4%)
and
multivitamins
(20.5%).
Similarly,
39
(63%)
pharmacies
had
refrigerators
to
keep
the
important
medicines
in
cool
environment
but
only
2
(3%)
pharmacies
had
temperature-monitoring
devices
(Table
4).
None
of
the
pharmacies
had
a
cold
storage
facility
other
than
the
refrigerator.
Table
4:
Findings
regarding
the
temperature
of
community
pharmacies
(Objective
assessment)
(n=62)
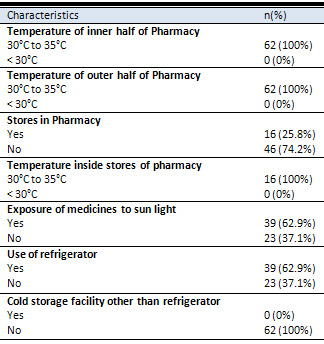
Out
of
62
pharmacy
owners,
16
(26%)
had
a
separate
storage
area
within
the
main
pharmacy
and
in
these
areas
the
temperature
was
found
to
be
more
than
25
°C.
Approximately
8
(13%)
pharmacy
owners
reported
that
the
store
is
large
enough
to
keep
all
the
supplies.
Around
11
(18%)
pharmacies
had
a
storage
room
which
was
reserved
only
for
pharmacy
related
functions,
and
7
(11%)
had
adequate
storage
capacity
in
the
warehouse
for
medicines
and
medical
supplies.
Moreover,
in
6
(10%)
pharmacies,
the
stores
were
in
good
condition.
One
(2%)
pharmacy
was
found
to
have
a
store
with
cracks,
holes
and
signs
of
water
leakage.
In
9
(15%)
pharmacies,
the
stores
had
a
ceiling
in
from
which
5
(8%)
were
not
in
good
condition.
In
2
(3%)
pharmacies,
the
stores
were
properly
ventilated
with
appropriate
air
entry.
Stores
of
7
(11%)
pharmacies
were
tidy
with
clean
shelves,
walls
and
did
not
have
signs
of
any
infestation.
Furthermore,
15%
of
the
stores
did
not
have
any
expired
items
in
their
storage
area
(Table
5).
Table
5:
Findings
regarding
storage
of
medicines
in
separate
storage
area
of
main
Pharmacy
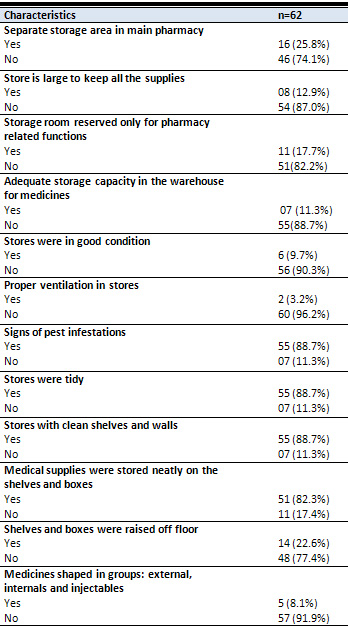
Medical
supplies
were
stored
neatly
on
the
shelves
and
boxes
in
82%
of
the
pharmacies
but
shelves
and
boxes
were
raised
off
the
floor
in
only
23%
of
the
pharmacies.
In
5
(8%)
pharmacies,
the
supplies
were
categorized
in
various
groups.
None
of
the
pharmacy
owners
had
practice
of
storing
the
controlled
substances
in
double
locked
storage
space
(Table
5).
Exposure
of
medicines
to
high
temperature
in
storage
or
in
transport
could
reduce
their
efficacy
of
drugs
including
vaccines(11).
The
major
factors
which
contribute
to
decreased
efficacy
of
medicines
after
quality
manufacturing
are
improper
storage
of
medicines
at
undesirable
temperature
(22).
The
journey
of
medicines
begins
at
the
site
of
manufacturer
and
passes
through
warehouses,
pharmacies
and
sometimes
other
environments
before
reaching
the
end
user
(20).
Temperature
conditions
in
earlier
stages
have
received
attention,
but
little
work
has
been
done
in
primary
care
settings
and
community
pharmacy
settings,
both
in
developed
and
developing
countries
(20).
The
findings
of
present
study
suggest
that
majority
of
pharmacy
owners
had
knowledge
about
correct
temperature
for
storing
medicines
at
that
temperature
(<25?C)
but
almost
100%
of
the
community
pharmacies
were
having
temperature
(>25?C)
degree
centigrade,
which
is
more
than
the
required
temperature
for
storing
medicines
safely.
In
both
environments
i.e.
outer
and
inner
half
of
pharmacies,
medicines
were
exposed
to
temperature
greater
than
(>25?C).
These
findings
suggest
that
there
is
huge
gap
between
knowledge
of
pharmacy
owners
and
their
practices
because
on
one
hand
they
highlighted
that
high
temperature
(>25?C)
can
affect
quality
of
medicines
and
on
other
hand
temperature
control
at
required
level
(<25?C)
is
not
ensured
in
community
pharmacies
of
these
rural
areas.
Moreover,
these
findings
are
supported
by
the
fact
that
medicines
were
directly
exposed
to
sunlight
in
63%
of
the
community
pharmacies.
These
findings
are
consistent
with
other
studies
around
the
world
(20).
Our
study
also
examined
storage
practices
in
the
community
pharmacies.
Although,
63%
of
the
pharmacies
had
a
refrigerator
to
keep
the
medicines
in
a
cool
environment
but
due
to
incessant
electricity
shut
downs
(estimated
to
be
approximately
12
hours
per
day),
and
limited
backup
power
supply,
may
render
these
medicines
ineffective.
Our
study
reveals
that
3%
of
the
pharmacies
were
having
a
temperature
monitoring
facility
or
device.
With
a
dearth
of
temperature
monitoring
devices,
excessive
electric
cut-offs
and
limited
alternative
power
supply
for
refrigeration,
and
may
potentiate
doubt
on
the
efficacy
of
medicines.
These
findings
were
consistent
with
that
reported
from
Banglore,
India
(27).
These
findings
of
having
refrigerator
and
temperature
monitoring
facility
were
slightly
different
from
the
study
findings
conducted
by
Zahid
A
Bhutt
et
al
in
Urban
Rawalpindi
in
2005,
where
majority
(76%)
of
the
pharmacy
owners
had
refrigerator
and
10%
of
these
pharmacies
had
temperature
monitoring
devices
as
well(28).
The
difference
in
findings
of
having
refrigerator
in
current
study
might
be
due
to
setting
of
the
study
in
the
rural
district
of
Sindh
where
worth
of
purchasing
refrigerator
might
not
be
considered
as
compared
to
urban
areas.
Moreover,
due
to
frequent
electricity
cut-
offs,
pharmacy
owners
might
not
prefer
to
invest
in
purchasing
the
refrigerator
or
they
might
not
have
the
knowledge
of
keeping
the
required
medicines
in
the
refrigerator.
Around
25%
of
the
pharmacies
were
selling
vaccines
and
all
of
these
pharmacies
were
storing
the
vaccines
in
refrigerator,
despite
limitations
of
maintaining
the
desired
temperature.
These
findings
were
different
from
the
studies
conducted
in
Karachi
and
Rawalpindi,
where
more
than
half
of
the
pharmacy
owners
were
selling
vaccines
irrespective
of
appropriate
storage
practices(28,
29).
This
difference
might
be
due
to
difference
in
demand
and
supply
of
rural
and
urban
areas.
In
urban
areas,
community
people
might
be
aware
about
and
might
give
high
importance
of
preventive
aspect
of
the
health
therefore
there
would
be
more
demand
for
vaccines,
which
might
be
satisfied
by
equal
supply
by
community
pharmacies
in
urban
areas.
Furthermore,
our
study
also
found
that
commonly
used
medicines
like
NSAIDs,
multivitamins
and
antibiotics
were
exposed
to
direct
sunlight
and
studies
have
also
shown
that
such
medicines
show
significant
reductions
in
activity
when
stored
at
temperature
more
than
25oC
(20).
Furthermore,
studies
have
also
shown
that
dissolution
rate
of
diclofenac
sodium
(NSAIDs)
tablets
significantly
reduces
in
as
little
as
three
months
following
exposure
to
high
ambient
temperature(20).
Although
the
community
pharmacy
owners
had
knowledge
about
the
adverse
effects
of
high
temperature
on
medicines
but
they
could
not
modify
the
temperature
of
community
pharmacies
alone
due
to
multiple
barriers
like
lack
of
air
conditioning
system,
load
shedding
problems
and
lack
of
backup
power
supply
in
community
pharmacies.
Moreover,
there
might
be
other
barriers
or
factors
which
might
have
stopped
community
pharmacy
owners
or
drug
sellers
to
maintain
the
required
temperature
in
their
respective
pharmacies
and
there
is
strong
need
to
explore
such
barriers
in
future
studies.
Since
pharmacies
are
often
the
first
point
of
interaction
for
patients
looking
for
health
care
as
they
are
usually
more
reachable
and
less
socially
distant
than
other
health
care
providers,
including
general
physicians
and
consultants.
Therefore,
if
drugs
or
vaccines
are
compromised
by
quality
issues
such
as
improper
storage
of
medicines
at
undesirable
temperature
then
community
people
may
end
up
with
products
or
instructions
that
are
useless
and
even
dangerous
for
the
community
as
a
whole(28).
In
fact,
it
has
been
said
that
if
a
physician's
medical
error
could
terminate
a
life,
then
a
singular
error
from
the
drug
manufacturer
or
dealer
can
most
certainly
lead
to
the
loss
of
many
lives(30).
| STRENGTHS
AND
LIMITATIONS
OF
THE
STUDY
|
There
is
a
scarcity
of
literature
regarding
the
storage
practices
of
medicines
in
community
pharmacies,
particularly
in
rural
areas
of
Pakistan.
Therefore,
to
the
best
of
our
knowledge
this
was
the
first
study
of
its
kind
that
has
assessed
the
temperature
and
storage
practices
of
medicines
in
community
pharmacies
in
rural
district
of
Sindh,
Pakistan.
Temperature
was
measured
objectively
with
the
standard
procedure
to
avoid
the
measurement
bias.
In
addition
to
this,
study
findings
can
be
generalized
to
rural
areas
of
developing
countries.
The
scope
of
this
study
was
limited
to
pharmacy
owners
and
drug
inspectors
but
perceptions
of
owners
of
pharmaceutical
companies,
other
government
authorities,
community
stakeholders
and
policy
makers
could
not
be
assessed.
The
collection
of
data
was
limited
to
only
two
talukas.
Interviewer
bias
might
be
there
due
to
nature
of
questions
being
asked
from
pharmacy
owners.
The
study
found
more
than
a
quarter
of
pharmacy
owners
had
knowledge
about
maintaining
the
required
temperature
of
<
25°C
but
none
of
the
pharmacies
in
the
catchment
area
were
maintaining
required
temperature
of
<
25°C.
We
also
concluded
that
storage
practices
in
community
pharmacies
/
medicine
stores
were
found
to
be
poor
and
very
few
pharmacy
owners
were
monitoring
temperature
in
their
pharmacies.
Although
there
were
some
observed
insignificant
cases
of
satisfactory
storage
practices
amongst
community
pharmacies/
medicine
stores,
nevertheless
the
evidently
generally
poor
storage
practices
weighed
higher
because
of
their
potential
untoward
chain
effects
on
drug
consumers.
Moreover,
looking
at
the
median
duration
of
load
shedding
and
limited
backup
power
supply,
it
is
very
important
to
make
cost
effective
and
long
lasting
strategies
to
maintain
the
safety,
efficacy
of
medicines
and
to
improve
quality
of
medicines
especially
in
remote
areas.
Strict
monitoring
and
regulation
of
these
pharmacies
are
required.
Such
storage
practices
should
also
be
evaluated
at
homes
to
see
that
how
people
store
these
medicines
in
their
households.
Furthermore,
there
is
a
need
to
enforce
existing
legislation
with
ongoing
training
programs
directed
towards
pharmacy
owners
and
drug
sellers
and
to
involve
the
pharmaceutical
industry,
which
plays
an
important
role
in
influencing
pharmacy
practices
of
pharmacy
owners.
In
future,
more
research
is
required
to
explore
the
different
ways
of
maintaining
the
required
storage
conditions
of
medicines
to
ensure
the
adequate
efficacy,
safety
and
effectiveness
of
medicines.
1.
Butt
ZA
GA,
Nanan
D,
Sheikh
AL,
White
F.
Quality
of
pharmacies
in
Pakistan:
a
cross-sectional
survey.
International
Journal
for
Quality
in
Health
Care.
2005;17(4):307-13.
2.
Hafeez
A,
Kiani
AG,
Din
Su,
Muhammad
W,
Butt
K,
Shah
Z,
et
al.
Prescription
and
Dispensing
Practices
in
Public
Sector
Health
Facilities
in
Pakistan-Survey
Report.
JOURNAL-PAKISTAN
MEDICAL
ASSOCIATION.
2004;54(4):187-91.
3.
Thome
J-M
PSL.
People's
Democratic
Republic:
health
financing
reform
and
challenges
in
expanding
the
current
social
protection
schemes.
Promoting
Sustainable
Strategies
to
Improve
Access
to
Health
Care
in
the
Asian
and
Pacific
Region.
2009:71-102.
4.
Du
B,
Daniels
VR,
Vaksman
Z,
Boyd
JL,
Crady
C,
Putcha
L.
Evaluation
of
physical
and
chemical
changes
in
pharmaceuticals
flown
on
space
missions.
The
AAPS
journal.13(2):299-308.
5.
Abegunde
D.
Essential
Medicines
for
Non-Communicable
Diseases
(NCDs)
and
pharmaceutical
policies
by
WHO.
2013.
6.
Butt
ZA,
Gilani
AH,
Nanan
D,
Sheikh
AL,
White
F.
Quality
of
pharmacies
in
Pakistan:
a
cross-sectional
survey.
International
Journal
for
Quality
in
Health
Care.
2005;17(4):307-13.
7.
Azhar
HUSSAIN
MIMI.
Qualification,
knowledge
and
experience
of
dispensers
working
at
community
pharmacies
in
Pakistan
Original
Research.
may
2011.
8.
Bott
RF,
Oliveira
WP.
Storage
conditions
for
stability
testing
of
pharmaceuticals
in
hot
and
humid
regions.
Drug
development
and
industrial
pharmacy.
2007;33(4):393-401.
9.
Pau
AK,
Moodley
NK,
Holland
DT,
Fomundam
H,
Matchaba
GU,
Capparelli
EV.
Instability
of
lopinavir/ritonavir
capsules
at
ambient
temperatures
in
sub-Saharan
Africa:
relevance
to
WHO
antiretroviral
guidelines.
Aids.
2005;19(11):1233.
10.
Hogerzeil
HV,
Battersby
A,
Srdanovic
V,
Stjernstrom
NE.
Stability
of
essential
drugs
during
shipment
to
the
tropics.
BMJ:
British
Medical
Journal.
1992;304(6821):210.
11.
Arshad
A,
Riasat
M,
Mahmood
MKT.
Drug
Storage
Conditions
in
Different
Hospitals
in
Lahore.
Journal
of
Pharmaceutical
Sciences
and
Technology.3(1):543-47.
12.
Crichton
B.
Keep
in
a
cool
place:
exposure
of
medicines
to
high
temperatures
in
general
practice
during
a
British
heatwave.
JRSM.
2004;97(7):328-9.
13.
Mahbub-ul-Haq.
Human
Development
in
South
Asia,Oxford
University
Press.
Karachi;
1998.
14.
Corelli
RL,
Zillich
AJ,
de
Moor
C,
Giuliano
MR,
Arnold
J,
Fenlon
CM,
et
al.
Recruitment
of
community
pharmacies
in
a
randomized
trial
to
generate
patient
referrals
to
the
tobacco
quitline.
Research
in
Social
and
Administrative
Pharmacy.9(4):396-404.
15.
Rafie
S,
Kim
GY,
Lau
LM,
Tang
C,
Brown
C,
Maderas
NM.
Assessment
of
Family
Planning
Services
at
Community
Pharmacies
in
San
Diego,
California.
Pharmacy.1(2):153-9.
16.
Farris
KB
F-LF,
Benrimoj
SIC.
Pharmaceutical
care
in
community
pharmacies:
practice
and
research
from
around
the
world.
Annals
of
Pharmacotherapy.
2005;39(9):1539-41.
17.
Adepu
R
NB.
General
practitioners\'
perceptions
about
the
extended
roles
of
the
community
pharmacists
in
the
state
of
Karnataka:
.
A
study
Ind
J
Pharma
Sci.
2006;
68:
36-40.
18.
Organization.
WH.
Role
of
Dispensers
in
Promoting
Rational
Drug
Use.
2000
19.
Qidwai
W
et
al.
Private
drug
sellers
education
in
improving
prescribing
practices.
J
Col
Physic
Surg
Pak
2006
16:
743-6.
20.
Viberg
N.
Selling
Drugs
or
Providing
Health
Care?:
The
role
of
private
pharmacies
and
drugstores,
examples
from
Zimbabwe
and
Tanzania.
Institutionen
fÃr
folkhälsovetenskap/Department
of
Public
Health
Sciences;
2009.
21.
Jacobs
S,
Hassell
K,
Ashcroft
D,
Johnson
S,
O’Connor
E.
Workplace
stress
in
community
pharmacies
in
England:
associations
with
individual,
organizational
and
job
characteristics.
Journal
of
health
services
research
&
policy.19(1):27-33.
22.
Bell
KN,
Hogue
CJR,
Manning
C,
Kendal
AP.
Risk
factors
for
improper
vaccine
storage
and
handling
in
private
provider
offices.
Pediatrics.
2001;107(6):e100-e.
23.
Patel
KT,
Chotai
NP.
Pharma
science
monitor.
Int
J
Pharm
Sci.1980-93.
24.
NoorAli
R,
Luby
S,
Rahbar
MH.
Does
use
of
a
government
service
depend
on
distance
from
the
health
facility?
Health
policy
and
planning.
1999;14(2):191-7.
25.
World
Health
O.
hepatitis
B.
2002.
26.
Enemuor
SC,
Atabo
AR,
Oguntibeju
OO.
Evaluation
of
microbiological
hazards
in
barbershops
in
a
university
setting.
Scientific
Research
and
Essays.
2012;7(9):1100-2.
27.
Sudarshan
MK
SM,
Girish
N,
Narendra
S,
Patel
NG.
An
evaluation
of
cold
chain
system
for
vaccines
in
Bangalore.
Indian
J
Pediatr.
1994;61:173-8.
28.
ZAHID
A.
BUTT
AHG,
DEBRA
NANAN,
ABDUL
L.
SHEIKH
AND
FRANK
WHITE.
Quality
of
pharmacies
in
Pakistan:
a
cross-sectional
survey.
International
Journal
for
Quality
in
Health
Care.
2005;17(4):307-13.
29.
Rabbani
F
CF,
Talati
N.
Behind
the
counter:
pharmacies
and
dispensing
patterns
of
pharmacy
attendants
in
Karachi.
Journal
of
Pakistan
Medical
Association.
2001;51:149-54.
30.
N.
C.
Obitte
AC,
D.
C.
Odimegwu
and
V.C.
Nwoke.
Survey
of
drug
storage
practice
in
homes,
hospitals
and
patent
medicine
stores
in
Nsukka,
Nigeria.
Scientific
Research
and
Essay.
November,
2009;4(11):1354-9.
|

