|
Quality of Life and its predictors
among Qatari Elderly Attending Primary Health
Care Centers in Qatar
Maha
Hammam Alshamali
(1)
Mohamed M. Makhlouf (2)
Mervat Rady (3)
Nagah Abdel Aziz Selim (4)
Mansoura Fawaz Salem Ismail (5)
(1) Supervisor of Disease Control Program,
Ministry of Health, Qatar
(2) Professor of Geriatric Health, High Institute
of Public Health, Alexandria University, Egypt
(3) Professor of Public Health, Faculty of Medicine,
Ain Shams University, Egypt
(4) Consultant Physician of Public Health and
Preventive Medicine, Asst. Director of Community
Medicine residency program, Primary Health Care
Corporation, Qatar, Asst. Professor of Public
Health and Preventive Medicine, Faculty of Medicine,
Cairo University
(5) Asst. Professor of Family Medicine, Faculty
of medicine, Suez Canal University Egypt , Family
Medicine Dept.
Corresponding Author:
Dr Mansoura Fawaz Salem
Assistant Professor of Family Medicine, Faculty
of Medicine, Suez Canal University,
Egypt
Family Medicine Consultant at Primary Health
Care Corporation,
Qatar
Mobile number: 0097450013135
Email: mansoura70@hotmail.com
Received: June 2018; Accepted: April 2019;
Published: May, 2019. Citation: Maha Hammam
Alshamali, Mansoura Fawaz Salem et al. Quality
of Life and its predictors among Qatari Elderly
Attending Primary Health Care Centers in Qatar.
World Family Medicine. 2019; 17(6): 9-19. DOI:
10.5742MEWFM.2019.9365
|
Abstract
A
cross-sectional study was conducted at
14 randomly selected Primary Health Care
Centers in Qatar to assess QOL and some
of its determinants among 672 Qataris
aged 60 years or more. Convenience cluster
sampling technique, and an Arabic structured
interviewing questionnaire were used.
QOL was assessed using an Arabic version
of the WHO-BREF questionnaire with a tested
specific QOL-old add-on module; the higher
the domains and total scores, the better
the QOL.
Results:
Around three quarters of males had good
to very good QOL, while nearly the same
percentage of females had fair to poor
QOL. All the elderly had from fair to
very good ADL% and most of them were in
the fair/good level for the IADL%. Social
activity was significantly correlated
with QOL. Gender, educational level, income
sufficiency, number of chronic diseases,
perceived general health and IADL% were
the significant predictors for the total
QOL.
Conclusion:
QOL among the participants was average.
Physical domain had the highest mean score,
while the social domain had the lowest.
Gender and chronic co-morbidities, were
significant predictors of elderly QOL.
Key words:
elderly, quality of life, Qatar
|
Aging populations have become a leading demographic
issue in the new millennium. There has been
a rapid increase in the elderly population all
over the world. By 2050, the world’s population
aged 60 years and older is expected to total
2 billion, up from 841 million today, and it
will be the first time in history where the
number of people aged 60 years and older, outnumber
children younger than 5 years [1]. The challenge
for aging studies is to understand the conditions
associated with aging as a positive process
and old age as a stage of life in which health,
well-being, pleasure and quality of life (QOL)
can be increased [2]- [4]. While population
aging in the Arab region is not currently of
the order of magnitude witnessed in some developed
countries such as Japan or Korea, it has already
started in a number of Arab countries and is
expected to gather momentum in the next 50 years.
Despite this fact, most Arab countries appear
to underestimate the importance of this issue
and are not anticipating the future repercussions
on national economies caused by this demographic
transition.
In Qatar, the number of people aged 60 years
or more is expected to increase from 17,500
(3.1%) in 2000 to 172,000 (20.7 %) in 2050,
a 10-fold increase [5]. Despite the support
that medical and social systems provide to the
elderly, many older people still experience
discomfort because of loneliness, depression,
social isolation, or constrained quality of
life [6]. The QOL of older adults could be good,
or at least preserved, provided they have autonomy,
independence and good physical health and provided
they fulfill social roles, remain active and
enjoy a sense of personal meaning [7]. QOL as
a person’s sense of well-being is not homogeneous
but is multidimensional, with many components
that range from health indicators to individual
habits, culture and ethics [8]. Personal opinions
should therefore be taken into account when
assessing elderly QOL [9]. Health interventions,
welfare programs, health care and the well-being
of the elderly can be improved and evaluated
through studies of their QOL. The World Health
Organization (WHO) defines QOL as an individual’s
perception of his/her status in life in the
context of the individual’s environment,
belief systems, and goals [10]. Several studies
have shown that younger elderly, being married
or females with adequate income are likely to
have better QOL in comparison to older elderly,
males, divorced or widows with inadequate income
[11-15]. Moreover elderly people with higher
education were found to have a better QOL than
those with lower education [ 16]. Furthermore,
an active lifestyle preserves physical function
in older adults which may possibly contribute
to higher levels of QOL scores in domains related
to physical health [17].
Evaluating elderly QOL should be done from
a different perspective to QOL assessments for
the general population [18]. In spite of this,
there is still a lack of studies directed towards
aging in general and elderly QOL in particular,
for the population of Qatar. This study assesses
QOL and its different domains among a group
of elderly Qataris visiting primary health care
(PHC) centers in Qatar and seeks to identify
determinants of QOL.
Study design: A cross-sectional study
Setting: The study was conducted in
14 health centers out of 21 PHC centers distributed
throughout Qatar.
Sample Size & Technique: Subjects
included male and female elderly Qataris aged
60 years or more who visited the PHC centers
during the 3 month’s field work duration
from March 15 to June 15, 2015. Consent was
gained to participate in the study. Convenience
cluster sampling technique with proportional
allocation was used. The estimated sample size
was 672 elderly individuals based on prevalence
of bad QOL = 24% (from pilot study results),
95 confidence interval, precision = 5%, design
effect = 2, and inflation rate = 20%. Data collection
in each center was carried out on a daily basis
until the required quota from each center was
reached.
Inclusion criteria: All Qatari elderly
aged 60 years or more, males and females who
visited the health centers during the study
field work, were invited to participate.
Exclusion criteria: Individuals below
60 years of age or with communication problems
or with a score < 7 as screened by the Short
Portable Mental Status Questionnaire (SPMSQ),
indicating severe cognitive affection, were
excluded [19].
Method of data Collection tool: The
study tool was an Arabic structured interview
questionnaire including the following items:
(a) Socio-demographic data such as age, sex,
income level, educational level and marital
status.
(b) Health measures such as types of chronic
diseases, hospital admissions, current medications
and screening questions for depression.
(c) Assessment of QOL by the WHOQOL-BREF standard
questionnaire (Arabic version) [20], with an
add-on old module for elderly populations. The
questionnaire has 26 items on a 5-point scale,
ranging from totally absent/totally disagree/very
bad to totally present/totally agree/excellent;
it also included 2 subjective overall items
allowing the subject’s self-evaluation
of his/her overall QOL and overall health, as
well as 24 items relating to 4 domains: physical
health, psychological well-being, social and
environmental domains. From those questions,
2 were excluded; this included questions about
working capacity, since all elderly were retired
and jobless, and that relating to sexual activity,
as it was totally missing in the responses.
The scoring rules for the questionnaire assessment
were followed according to the WHOQOL group;
questions 3, 4, and 26 were reversed, as they
were negative questions. The add-on old module
is a short form of the original 24-question
WHOQOL-OLD questionnaire [21]; it includes only
6 questions, 1 from each of the 6 facets. Each
question was rated on a Likert scale ranging
from 1–5, where 1 represents never and
5 represents always. The sum of its scores ranges
from 6–30, and the total number of questions
was 2 (global) + 22 WHOQOL + 6 Old domain =
30 questions. The total QOL score was calculated
by the sum of all the domain scores, giving
a range from 30–150. In each domain and
in the total QOL, higher scores indicated better
QOL. The raw score for each domain and the total
score were converted into percentages for international
comparisons, because the add-on module prevented
direct score comparison with the WHOQOL-100.
The three percentiles (25th = 91, 50th = 100,
75th = 108) were used to categorize total QOL
scores as poor QOL (< 91), fair (91–99),
good (100–107), and very good (> 107).
Each domain was analyzed separately, as was
the total QOL against the independent variables.
(d) Social activities were assessing elderly
weekly participation in social activities including
going to pray, social gathering and playing
games. The responses were coded as (1-never
/ 2- 1-2 times per week / 3- 3-6 times per week/
4-daily). Also the frequency of attending other
social activities such as marriage parties,
funerals and ceremonies was also inquired about
and the responses were coded as (1- never 2-
rarely 3- sometimes 4-usually). Answers of these
5 questions were given a score (1) for never
response to (4) for daily/usually response.
The scores transformed into percent on the scale
from 0-100% [22].
e) Functional abilities were assessed by a validated
Arabic version of Katz index for activities
of daily living (ADL) [23] and Lawton scale
for instrumental activities of daily living
(IADL) [24]. For ADL, 6 functions were enquired
about: bathing, dressing, toileting, transporting,
continence and feeding. Three weighted categories
were used to evaluate the elderly’s response:
(1) totally independent, (2) partially independent
(3) totally dependent. For IADL, 8 functions
were enquired about: 6 common for both males
and females and including : the ability of using
a telephone, going out more than walking distance,
shopping, managing money, preparing meals, housekeeping,
laundry and taking medications without assistance.
Three weighted categories were also used to
evaluate the elderly’s response: (1) totally
independent, (2) partially independent and (3)
totally dependent. A pilot study was conducted
among 30 elderly Qataris in order to make adjustments
before the actual study commenced.
Data analysis: The data were analyzed
using Statistical Package of Social Science
[SPSS] version 20. Data normality was tested
using the K–S test and histograms. Descriptive
analysis was calculated in the form of mean
with SD for parametric quantitative variables,
median and IQR for non-parametric variables,
and frequency and % for qualitative data. Chi-square
and Fisher’s exact tests were used to examine
the relationship between qualitative variables,
while Student’s t-test and ANOVA with post-hoc
LSD were used for normally distributed quantitative
variables. The Mann–Whitney U test was
used for non-parametric quantitative variables.
Pearson or Spearman correlations were used for
bivariate correlations according to data normality.
Multiple regression analysis was done. All the
predictive risk factors significantly associated
with each domain of QOL were entered into the
final total QOL multiple linear regression model.
This model was used to identify the QOL predictors,
and p < 0.05 was considered statistically
significant.
Ethical Consideration: Institutional
Review Board (IRB) was obtained from Hamad Medical
Corporation. Informed consent was obtained from
each participant. Voluntary participation and
confidentiality were assured.
Among
the
672
elderly
included
in
the
study,
54.2%
were
male.
There
was
no
significant
difference
in
the
mean
age
between
males
and
females.
The
majority
of
the
subjects
were
currently
married
(78.9%),
71%
were
illiterate;
most
participants
were
retired
and
99%
were
on
a
pension
and
78%
reported
that
their
income
was
not
sufficient
,
all
participants
had
a
history
of
chronic
disease.
About
70%
of
the
female
elderly
had
3
diseases
or
more
compared
to
only
60.4%
among
males.
Hospital
admissions
in
the
year
prior
to
the
study
period
were
reported
by
11.8%,
with
no
significant
difference
between
males
and
females.
It
was
reported
that
63%
of
females
were
using
3
or
more
medications
compared
to
47%
among
males;
this
was
a
highly
significant
difference
(p
<
0.001).
The
most
prevalent
reported
disease
was
diabetes
mellitus
(88.8%),
which
was
more
common
among
females
(94.5%)
than
males
(84.1%);
followed
by
hypertension
(69.3%),
which
was
more
common
among
males
(74.5%)
than
females
(63.3%),
and
then
raised
blood
lipids
(66.5%),
which
was
more
common
among
females
(70.5%)
than
males
(63.2%);
these
differences
were
all
statistically
significant
(Table
1).
Click
here
for
Table
1:
Socio-demographic
characteristics
and
self-reported
medical
history
among
the
elderly
Qataris
attending
Primary
Health
Care
Centers
in
Qatar,
(n
=
672)
Table
2
shows
that
the
mean
score
of
social
activity
was
equal
to
38.7
±
18.1
for
the
whole
study
participants
with
higher
mean
score
%
among
males
being
49.0
±
15.9
while
that
of
the
females
was
26.5
±
11.9
and
the
difference
was
highly
significant
since
p<
0.001.
The
total
mean
score
%
of
functional
abilities
ADL;
was
4.2
±
12.1
while
that
of
the
IADL
was
44.3
±
17.2.
The
mean
%
score
for
both
the
ADL
and
IADL
highly
significantly
differed
between
males
and
females.
Males
were
more
independent
with
lower
mean
scores
%
being
1.05
±
4.95
and
34.68
±
13.5
respectively
while
females
were
more
dependent
with
higher
mean
scores
%
being
7.98
±
16.27
and
55.69
±
13.92
respectively.
As
shown
in
Table
3,
the
highest
domain
percentages
were
for
the
environmental
and
social
domains
(71%
each),
followed
by
the
physical
health
(65%)
and
the
psychological
domain
(64%).
The
lowest
score
was
for
the
QOL-old
domain
sum
items
(47.5%).
A
combined
51%
of
the
elderly
enjoyed
a
very
good
or
good
QOL
(24.9%
and
26.1%,
respectively),
while
49%
had
a
fair
or
poor
QOL
(24.1%
and
24.9%,
respectively;
Figure
1).
Table
2:
Social
activity
and
functional
abilities
of
the
elderly
attending
Primary
Health
Care
Centers
in
Qatar,
(n
=
672)
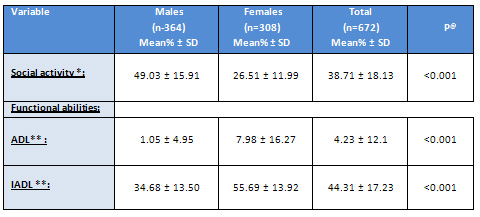
*
The
higher
the
mean
%,
the
higher
the
Social
activity
**
The
higher
the
mean
%,
the
lower
function
and
higher
dependency
@
Using
Mann
Whitney
U
test
Click
here
for
Table
3:
Description
of
total
QOL,
its
domains,
perceived
overall
QOL,
and
perceived
overall
health
among
elderly
visiting
Primary
Health
Care
Centers
in
Qatar(n
=
672)
Click
here
for
Figure
1:
Distribution
of
participants
according
to
QOL
grades
by
sex
(n
=
672)
All
the
domain
scores
were
tested
in
a
multiple
regression
analysis
model
to
predict
the
solo
contribution
of
each
domain
(Table
4).
It
revealed
that
the
physical
health
domain
had
the
highest
significant
impact
on
the
total
QOL
(36.1%),
and
the
social
domain
contributed
the
least
to
total
QOL
(8%).
The
perceived
overall
QOL
score
was
significantly
correlated
with
all
domain
scores
and
with
the
total
calculated
QOL
score.
All
the
correlations
were
statistically
significant
at
p
<
0.001.
The
strongest
correlation
with
perceived
overall
QOL
was
with
the
physical
health
domain
(r
=
0.72),
while
the
weakest
was
with
the
social
domain
(r
=
0.45).
Table
4:
Linear
regression
analysis
for
predicting
the
total
QOL
score
using
its
domains’
scores
as
independent
variables
for
the
elderly
visiting
Primary
Health
Care
Centers
in
Qatar(n
=
672)
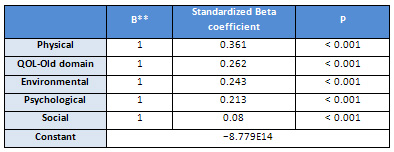
Dependent
variable:
total
QOL
R=1
R2=1
Adjusted
R2=1
**
100%
perfect
fit
model
Table
5
shows
the
statistically
significant
predictors
of
the
total
QOL
score
using
the
enter
model
for
multiple
linear
regression
analysis.
The
prediction
model
was
statistically
significant,
F
=
84.88,
p
<
0.001,
and
accounted
for
approximately
72%
of
the
variance
in
the
total
QOL
score
(R2
=
0.73,
adjusted
R2
=
0.72).
Other
than
the
gender,
educational
level
and
income
sufficiency,
all
the
other
demographic
factors
such
as
age
and
smoking,
were
found
to
be
insignificant
predictors
of
total
elderly
QOL.
Gender
was
the
main
socio-demographic
QOL
predictor,
contributing
11%
of
the
model
variance.
Among
health
factors,
the
remaining
significant
factors
in
the
model
were
the
number
of
chronic
diseases,
self-reported
overall
health,
osteoarthritis,
and
osteoporosis
by
29.3%,
27.2%,
8.3%,
and
6.8%,
respectively.
As
a
group,
health
factors
were
the
strongest
determinants
of
total
QOL.
Social
activity
is
a
predictor
of
the
total
QOL,
IADL%
was
also
a
significant
predictor
in
the
three
models.
As
a
group,
health
factors
were
the
strongest
determinants
of
the
total
QOL
for
the
three
models
followed
by
the
social
one.
Click
here
for
Table
5:
Statistically
significant
predictors
of
total
QOL
score
by
gender
using
the
enter
model
of
multiple
linear
regression
analysis
among
the
elderly
visiting
Primary
Health
Care
Centers
in
Qatar
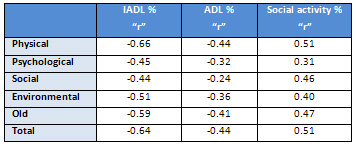
Table
6
shows
the
Spearman
correlations
between
the
QOL
domains
and
total
QOL%
scores
with
both
the
ADL%
and
the
IADL%
scores.
It
is
clear
from
the
table,
the
significant
negative
correlation
between
the
increase
in
inactivity
(higher
scores)
and
the
decrease
in
the
QOL
domains
%
scores
and
the
total
QOL%
score
with
P<0.001.
The
highest
negative
correlation
as
expected
was
observed
with
the
physical
health
domain
%
score
(r=-0.66
with
IADL
and
r=-0.44
with
ADL).
For
the
total
QOL
%
score,
the
IADL%
score
was
found
to
be
more
correlated
negatively
with
it
than
with
the
ADL%
score
(
r=
-64,
r=
-0.44
respectively)
and
the
same
result
was
observed
with
all
domains
%
scores.
As
regard
the
social
activity
and
its
effect
on
the
QOL,
it
was
found
to
be
correlated
positively
with
all
domain
%
scores
especially
the
physical
health
(r=0.51)
and
the
total
QOL
%
score
(r=0.51).
All
the
correlations
were
statistically
significant
at
p
<
0.001.
Table
6:
Spearman
correlation
between
Social
activities
score
%,
ADL
score
%,
ADL
score
%
and
QOL
domains
among
elderly
attending
Primary
Health
Care
Centers
in
Qatar,
(n
=
672)
*All
correlations
are
statistically
significant
at
p
<
0.001
NB:
there
is
a
significant
positive
correlation
between
IADL
%
score
and
ADL
%
score
;
r=
0.65
&
p<0.001
|

