Public
Assessment of Social and Economic Rehabilitation
Component of Leprosy Control Programmes in Anambra
and Ebonyi States of Southeast Nigeria
Nwankwo,
Ignatius Uche
Correspondence:
Nwankwo, Ignatius Uche, Ph.D.
Department of Sociology/Anthropology
Nnamdi Azikiwe University, Awka, Anambra State,
Nigeria
Email:
iunwankwo@yahoo.com
|
Abstract
Three major objectives informed this research
paper. The first was to find out the types
of social and economic rehabilitation
(SER) activities available to persons
affected by leprosy (PAL) in Anambra and
Ebonyi states of Southeast Nigeria. The
second is to find out the nature of public
perception on adequacy and outcomes of
social and economic rehabilitation packages
for leprosy cases, while the third is
to verify public view about adequacy or
otherwise of funding for social and economic
rehabilitation of persons affected by
leprosy in the two states. The study adopted
a cross-sectional survey design. Quantitative
data was generated through structured
questionnaire schedule administered on
1116 study participants. The participants
were selected through a combination of
cluster and simple random sampling methods.
Qualitative data were generated through
two instruments. These were Focus Group
Discussion (FGD) administered on persons
affected by leprosy and In-Depth Interview
(IDI) of leprosy control staff and officials
from both World Health Organization and
the donor agency supporting leprosy control
in the two states. The Statistical Package
for the Social Sciences (SPSS) software
was employed in analysis of data. Frequency
tables, percentages, bar charts, chi-square
and multiple regressions were used for
presentation, analysis and in testing
the stated hypotheses. It was found that
only 25.5% of the respondents acknowledged
availability of SER component which is
institutional rather than community based.
Furthermore, most respondents assessed
SER activities in leprosy control in the
two states as largely unsuccessful One
hypothesis test showed that more respondents
with low income perceived a link between
adequate funding and effective leprosy
control programme than those with higher
levels of income (X2=190.427,df=70,p=0.000).
It was recommended that aggressive public
enlightenment through public, private
and local media; incentive package for
health workers and extensive socio-economic
empowerment for effective rehabilitation
of patients be adopted to enhance leprosy
control in Anambra and Ebonyi states.
Key words:
Assessment, Leprosy, Leprosy Control,
Social and Economic Rehabilitation, Empowerment
|
Leprosy is one of the oldest diseases of mankind.
It has a unique social dimension that often
culminates in the total destabilization of the
social life of its victims. From the earliest
times, leprosy has been a disease set apart
from others. Its victims and even their care
givers are ostracised in many societies. Although
the disease seldom kills (Bryceson and Pfaltzgraff
1990), it remains a public health problem and
cause of morbidity especially in developing
countries like Nigeria. The disease is also
one of the leading causes of permanent disability
worldwide and has over the year's left a terrifying
memory of mutilation, rejection and social exclusion
(Lockwood, 2000). There are serious problems
confronting control programmes and victims of
leprosy in affected countries. In Nigeria, Sofola
(1999) expresses concern at poor funding of
leprosy control activities. There is also an
enormous problem of policy inconsistency in
the area of leprosy control. The initial emphasis
of control activities was on isolation of victims
at Leprosaria where specialist health staff
attend to them. The gains of this original focus
were as yet not fully tapped when a shift in
policy was initiated. According to Eboh (1999),
the old arrangement contributed to the difficulty
in achieving the present policy thrust of integrating
leprosy control programme with general primary
health care. It also resulted in the failure
of newer measures to attain optimal results,
since most people still adhere to the old practices.
Particularly disturbing is the graph below from
World Health Organization (WHO) Southeast of
Nigeria Office (2010), which shows that the
Southeast zone of Nigeria has consistently recorded
increases (rather than decreases) in both new
case detection and prevalence of leprosy since
2006-2009. This raises fundamental questions
about the potency of leprosy control programme
and whether leprosy should be classified as
a re-emerging disease in the area and for what
reasons.
Figure 1: Leprosy New Case Detection (NCD)
and Prevalence, 2005 - 2009 for South-east Zone
of Nigeria
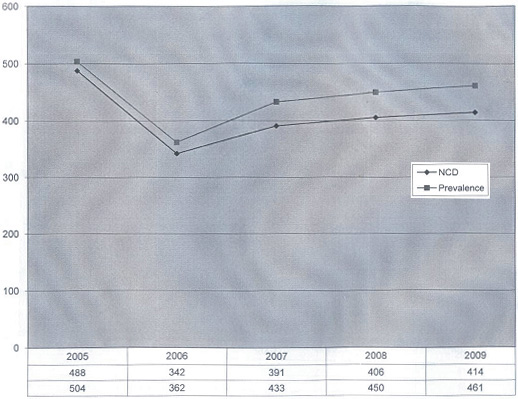
Source: World Health Organisation, Southeast
Zonal Office, Enugu Nigeria, (2010).
Furthermore, poor leprosy control outcomes have
persisted to the extent that a former World
Health Organization's Country Representative
in Nigeria, Dr Peter Ekiti lamented that in
2008; only 14% of the estimated new leprosy
cases in Nigeria were actually detected and
enrolled for treatment (Ekiti, 2010). Similarly,
Adagba (2011) and was very critical that prevalence
of leprosy among children in Nigeria is still
high and unacceptable.
In 2008, Nigeria was ranked at the fifth position
among nations with high leprosy burden in the
world, and in Africa, second only to Republic
of Congo (W.H.O, 2008). Nigeria's registered
prevalence of leprosy as at 2002 was 5890 (FMOH,
2004). It declined to 5381 by the beginning
of 2008 (W.H.O, 2008) and further to 3913 cases
at the end of 2010 (Adagba, 2011). The above
situation appears to be compounded by enormous
fear of leprosy among the Nigerian populace
(Ogoegbulem, 2000). In many parts of Nigeria,
despite the existence of leprosy control activities
since the pre-Dapsone era of 1900-1947, the
fear and stigma of leprosy remains high and
separates persons affected by leprosy (PAL)
from their fellows. Nicholls (2000) had similarly
observed that in both Eastern and Western cultures,
fear of leprosy has existed from ancient times.
On the other hand, Osakwe (2004) regretted
that community participation which is a crucial
element in leprosy control has remained weak
in Nigeria. Consequently, community response
or behaviour toward those suffering from leprosy
is characterized by avoidance, insult and rejection
of victims. Even discharged leprosy ex-patients
are not spared of these actions that also constitute
violation of human rights.
Nicholls (2000) further observes that leprosy
more than any other disease has caused individuals
to leave their families and communities and
be forced to live as outcasts in separate colonies
and settlements. Some of such colonies or settlements
are still operating at Okija, Otolo-Nnewi, and
Amichi communities in Anambra state; and at
Mile Four Abakaliki and Uburu communities at
Ebonyi state. There are others at other parts
of Nigeria. Their continued operation is an
evidence of the failure of the National Leprosy
Control Programme to implement home based or
ambulatory care arrangement where most patients
access treatment from their homes, except those
who are in critical conditions and require hospitalization.
The advantage of home based care in reducing
segregation and facilitating the new thrust
toward Community Based Rehabilitation (CBR)
cannot be over-emphasized. Also problematic
is the fact that at such colonies, inmates live
in dilapidated structures surrounded by bushes
in more or less inhuman conditions. An integrated
and effective leprosy control programme has
a responsibility to provide conducive living
and treatment environment to persons affected
by leprosy. It should indeed address their bio-medical,
social and economic needs.
Accordingly, Smith (2000) notes that Social
and Economic Rehabilitation (SER) is a major
priority in any leprosy control effort. This
emphasis according to W.H.O (1999) is aimed
at addressing problems of stigmatization, inability
to work, social isolation and economic dependency.
However, Ogbeiwi (2005) reports that the SER
component of Nigeria's National Leprosy Control
Programme does not reflect the priority it deserves;
hence it is yet to make any appreciable impact.
Persons affected by leprosy in Southeast Nigeria
are already burdened by medical and bio-physical
challenges posed by the disease. Their having
to further contend with very serious social,
economic and psychological problems arising
from societal perception and consequent reactions
to their predicament are weighty. Ogoegbulem
(2000), reports that they often encounter severe
loss of dignifying self concept and social recognition.
They are not usually welcome at public functions.
On rare occasions where these patients or ex-patients
force themselves unto a gathering, this might
result either in an abrupt dismissal of participants
or in avoidance of any form of physical contact
with them. Indeed, Nigerians are afraid to sit
near persons affected by leprosy at churches,
markets, vehicles; village squares and so on.
They are also reluctant to marry from families
of known leprosy patients (Ogoegbulem, 2000).
The lack of friendship and other forms of association
as well as divorce or threats of divorce from
spouses constitute part of the numerous social
problems faced by persons affected by leprosy.
The control programme in Nigeria ought to find
answers to these myriad of problems.
In another development, the value of the use
of economic empowerment as a tool of leprosy
control has been extensively documented by scholars.
Examples of these are Nash (2001); Federal Ministry
of Health (FMOH, 1997); Macaden (1996); Pearson
(1988). However, Ogbeiwi (2005) notes that the
approach is yet to be adequately exploited in
Nigeria. This is despite the fact that the disease
is widely known to have devastating effect on
the economic life of its victims. For instance,
Rafferty (2005), notes that leprosy destroys
productivity of victims through series of disablement
or lack of physical function which it engenders.
The situation is complicated by the fact that
societies avoid goods and services offered by
persons affected by leprosy. Such poor patronage
tends to de-motivate the victims as it forces
them to abandon their trades.
In the light of the above and given the inadequacy
of economic support package from the control
programme, persons affected by leprosy often
resort to begging on the streets as means of
self-sustenance. Consequently, markets, bus-stops,
motor-parks, entrances to churches, banks and
offices are littered with these destitute. This
constitutes a threat to public health. It also
generates public outcry about the welfare of
persons affected by leprosy which the control
programme has a responsibility to protect.
The lukewarm attitude of health workers toward
leprosy control activities (Adagba, 2011) is
also a major challenge facing the control programme
Poor allowances, negative cultural reactions
towards leprosy and fear of contracting the
disease negatively affect the disposition of
health workers to committed service. Consequently,
the workers have not prosecuted aspects such
as public health education and ulcer dressing
in leprosy with sufficient zeal and enthusiasm.
Because of this, individuals and groups have
expressed deep concerns about poorly maintained
leprosy ulcers often exuding odorous discharges
and attracting flies which have become regular
feature of persons affected by leprosy. Leprosy
victims endure the pain of such ulcers as they
move about to solicit for alms. These patients
are also unsightly and degrade the aesthetic
beauty of neighbourhoods by their low level
of personal and environmental hygiene.
The gender dimension and social stratification
implications of leprosy are other areas which
the control programme is yet to adequately address.
The gender dimension of leprosy is such that
women encounter the severest forms of social,
economic and psychological consequences compared
to their male counterparts upon diagnosis of
leprosy (Kaur and Rameshi 1994; Grand 1997;
Rao, Garole and Walawalker 1996). Women do not
also occupy important positions in self help
groups formed by patients in their colonies.
This is especially so in a highly patriarchal
society like the South-eastern part of Nigeria
where subservient position and economic dependence
of women on men are culturally defined. Sofola
(1999), observes that in many leprosy colonies
in Nigeria, women affected by leprosy get smaller
portions of land for cultivation compared to
the males. Observation of the current situation
suggests that equality of the sexes in accessing
rights and privileges accruable from leprosy
control programme remains defective in Nigeria.
Valsa (1999) examined social acceptance and
social stratification implications of leprosy.
He found that those affected could lose their
position in the social ranking of society. They
could be barred from taking important titles
or occupying positions of authority and honour.
They are not allowed to officiate important
occasions or to perform important rites associated
with such occasions even when it is their right
by birth in the community to do so (Kaufman,
Neville and Miriam, 1993; Ogoegbulem, 2000).
Expectations that leprosy control programme
in Nigeria would reverse the trend so far remains
a mirage. Above all, although WHO introduced
Multiple Drug Therapy (MDT) since 1985 as drug
of choice for leprosy (FMOH, 2008), it appears
that the treatment component of leprosy control
programmes have failed to respond to the needs
of persons affected by leprosy for cure or full
recovery without any deformity. The situation
is such that it is often difficult to distinguish
between victims who accessed treatment services
from those who did not due to permanent disabilities.
Also, their social and economic predicaments
are similar in most respects thus indicating
that the rehabilitation process of those who
accessed treatment services was not successful.
Ogoegbulem (2000) observes that victims of leprosy
who have completed treatment in parts of Nigeria
are not fully reunited and reintegrated into
the society and generally lack means of sustenance.
The seemingly resilient nature of leprosy and
its associated problems in Nigeria generate
doubts about the sincerity and commitment of
National Leprosy Control Programmes toward eradication
of leprosy by World Health Organization's global
target date. It is against the backdrop of the
above background and problems that the research
was undertaken to investigate public assessment
of social and economic rehabilitation component
of leprosy control programmes in Anambra and
Ebonyi states of Southeast Nigeria.
| BRIEF
REVIEW
OF
LITERATURE
ON
ROLE
OF
SOCIAL
AND
ECONOMIC
REHABILITATION
(SER)
IN
LEPROSY
CONTROL |
The role of rehabilitation
as one of the most important
aspects of leprosy control
has been emphasized
by several scholars
(see Nash 2001; Macaden
1996; Pearson 1988;
FMOH 1997). According
to Nash (2001), rehabilitation
of persons affected
by leprosy is a process
that helps them to feel
accepted, valued and
included in their community.
It assists them live
as normal a life as
possible. Pearson (1988)
defines it as the diagnosis,
treatment and prevention
of dehabilitation occasioned
by leprosy.
Rehabilitation for leprosy
patients usually involves
physical, social, economic
and psychological components
(FMOH, 1997). Pearson
(1988) gave reasons
for the multiple levels
of emphasis. He noted
that leprosy can cause
its victims to lose
physical forms, family
and place in society.
It can also cause them
to lose their work,
other means of livelihood
and their self respect.
These situations Pearson
says require detailed
rehabilitation response.
According to Macaden
(1996), rehabilitation
services for persons
affected by leprosy
could be organised in
three ways as follows:
a. Institution Based
Rehabilitation -
where patients lived
in and accessed rehabilitation
service only at the
health institution,
usually a Leprosarium.
Patients were not integrated
into their family or
community.
b. Outreach Services
- obtainable at camps,
outreach service points
and patient's home
c. Community Based
Rehabilitation (CBR).
This is the current
emphasis both in Nigeria
and globally (FMOH,1997).
It seeks not only to
help people overcome
their impairments, but
also to help them to
settle back fully in
their communities. CBR
in leprosy control adopts
an integrated approach.
It involves community
participation in provision
of rehabilitation services
to patients with diverse
social, economic, physical
and psychological needs
(FMOH, 1997).
Macaden (1996) similarly
stressed that CBR in
leprosy transfers to
members of the family
of the patient and the
community in which they
live, the skills needed
to manage physical impairments
and to provide vocational
training and placement.
On his part Nash (2001)
notes that the role
of community participation
in CBR is very crucial
to the extent that sometimes,
the community needs
as much rehabilitation
as the persons affected
by leprosy in order
to creditably discharge
their role in rehabilitation.
Smith (2000) also saw
social and economic
rehabilitation (SER)
of people affected by
leprosy as a major priority
that requires considerable
emphasis by control
programmes. This emphasis
according to W.H.O (1999),
is sequel to problems
of stigmatization, shame,
isolation, inability
to work or marry, dependency
on others for care and
financial support which
persons affected by
leprosy are exposed
to in many societies.
Nash (2001) reports
that in Nigeria, adherence
to guidelines on social
and economic rehabilitation
has been useful in restoration
of normal social and
economic life of persons
affected by leprosy.
He observed that preliminary
need assessment of patients
and active community
participation have ensured
that they fitted into
new socio-economic roles
like poultry keeping,
soap making, weaving,
tailoring, shoe-making
etc. Such roles he says,
restores social acceptance
and respect to patients.
Chukwu (2004) also looked
at the practice of CBR
in Nigeria. He commended
German Leprosy Relief
Association's support
towards social and economic
rehabilitation of persons
affected by leprosy
across fourteen states
in the Southeast and
Southwest of Nigeria.
He noted that the organization
has built houses, and
paid subsistence allowance
to patients. They have
also bought motorcycles
for public transport
services and given capital
to enable persons affected
by leprosy to start
their own businesses.
Despite these supports
by German Leprosy Relief
Association, Chukwu
(2004) insists that
contributions of the
rehabilitation arm of
leprosy control remains
insignificant across
most of Nigeria. According
to him, persons affected
by leprosy experience
various forms of discrimination
on account of the disease.
Many of them have no
means of subsistence
and depend on begging
to survive.
The
following
research
questions
guided
the
study:
(a)
What
types
of
social
and
economic
rehabilitation
programmes
are
available
to
persons
affected
by
leprosy
in
Anambra
and
Ebonyi
states?
(b)
What
are
the
perceived
outcomes
of
social
and
economic
rehabilitation
of
persons
affected
by
leprosy
in
Anambra
and
Ebonyi
states?
(c)
How
do
people
of
Anambra
and
Ebonyi
States
of
Southeast
Nigeria
perceive
the
level
of
funding
for
social
and
economic
rehabilitation
of
persons
affected
by
leprosy
in
their
area
in
terms
of
its
adequacy?
The
labelling
theory
is
relevant
in
explaining
the
problem
of
leprosy
in
the
study
area.
Labelling
theory
is
particularly
useful
in
the
analysis
of
the
qualitative
data.
This
is
because
of
its
emphasis
on
social
constructionism.
Labelling
theory
was
also
adopted
as
the
theoretical
platform
because
its
basic
postulations
explicitly
relate
to
the
process
of
social
definition
and
stigma
surrounding
leprosy.
These
are
central
issues
to
leprosy
problem
in
society.
Negative
cultural
imaging
of
leprosy,
and
the
manner
in
which
societies
through
the
instrument
of
language
defined
leprosy
as
a
curse
from
gods,
or
as
disease
of
the
unclean,
have
adverse
consequences
for
its
control.
People
are
reluctant
to
be
associated
with
the
disease
whether
as
patients
or
health
workers
because
of
the
stigma
attached
to
it.
It
is
therefore
not
surprising
that
despite
its
long
history
and
availability
of
free
and
effective
drugs
(FMOH,
2004),
leprosy
remains
a
public
health
problem
in
our
environment.
Adverse
religious
perspectives
on
leprosy
have
also
done
much
to
intensify
leprosy
stigma
and
worsen
problems
arising
from
leprosy
in
our
society.
Awofeso
(2005)
notes
that
biblical
references
like
Leviticus
13:45;
Numbers
5:2;
and
2
Kings
26:21
create
an
impression
that
leprosy
is
a
dreaded
disease
associated
with
sinners.
He
observes
also
that
Buddhist
teaching
on
Karma
make
it
acceptable
for
believers
to
frame
leprosy
sufferers
as
sinners
in
their
past
incarnation.
These
conceptions
compounded
by
low
level
of
education,
constitute
major
obstacles
to
leprosy
control.
Labeling
also
offers
adequate
explanation
to
why
persons
affected
by
leprosy
try
to
cover
up
their
disease
and
fail
to
avail
themselves
of
early
treatment.
The
situation
results
in
severe
deformities
and
complications.
The
theory
also
accounts
for
the
lack
of
enthusiasm
of
health
workers
to
leprosy
work,
and
for
low
level
of
integration
of
patients
into
their
community.
The
study
located
in
Anambra
and
Ebonyi
states,
randomly
selected
out
of
five
states
of
Southeast
Nigeria,
adopted
cross-sectional
survey
design.
The
Southeast
zone
of
Nigeria
was
purposively
selected
because
of
the
steady
increase
(rather
than
decrease)
in
number
of
leprosy
cases
registered
annually
in
the
zone
during
2006
-
2009
(see
Table
1
below).
Table
1:
Distribution
of
Leprosy
cases
according
to
States
in
the
Southeast
Zone
of
Nigeria
during
the
period
2006-2009
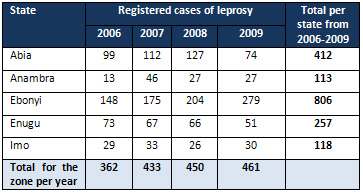
Source:
World
Health
Organisation,
Southeast
Area
Office,
Enugu
-
Nigeria,
(2010).Leprosy
New
Case
Detection,
Case
Detection
Rate
and
Prevalence
Rate
for
Southeast
Zone,
2006-2009.
The
indigenous
ethnic
group
in
the
two
states
are
the
Igbo
of
whom
Ifemesia
(1979)
observes
that
their
territory
covers
an
area
of
over
15,800
square
miles.
Nwala
(1985)
circumscribed
the
area
between
6o
and
8½o
East
longitude
and
4½o
and
7½o
North
latitude.
He
noted
that
Igbo
land
is
very
densely
populated.
Anambra
and
Ebonyi
states
are
rich
in
natural
resources
and
arable
soil.
Land
cultivation,
trading,
arts
and
crafts,
animal
husbandry
and
civil
service
are
major
economic
activities
in
the
two
states.
However,
people
of
Anambra
state
are
more
involved
in
entrepreneurship
and
commerce
whereas
Ebonyi
state
is
notable
for
agricultural
prowess
(Uzozie
2002;
Onokala
2002).
There
is
an
elected
civilian
government
in
Anambra
and
Ebonyi
states
whose
role
in
governance
of
the
area
is
complemented
by
socio-political
structures
and
pressure
groups
that
characterize
Igbo
traditional
societies
like
gerontocracy,
village
assembly,
titled
men,
women
groups
all
of
which
are
relevant
to
grass
root
administration
in
both
states.
Similarly,
Christianity
enjoys
greater
followership
in
the
area
but
exists
side
by
side
with
traditional
religion
which
still
has
many
adherents.
The
total
population
of
Anambra
and
Ebonyi
states
as
at
2006
national
population
and
housing
census
in
Nigeria
was
6,354,775
made
up
of
3,182,140
males
and
3,172,791
females.
However,
the
study
population
consisted
of
only
adults,
defined
as
persons
aged
18
years
and
above.
There
are
about
3,515,370
adults
in
the
area
which
represented
57.2%
of
the
total
population.
A
sample
size
of
1116
respondents
(558
from
each
state)
constituting
about
0.32%
of
the
study
population
was
used
to
generate
quantitative
data
in
this
study.
The
sample
was
adequate
for
applicable
statistical
tests.
The
sample
also
accommodated
geographical
spread
and
rural-urban
bias
at
the
ratio
of
2:1.
Qualitative
data
was
generated
from
64
respondents
made
up
of
52
persons
affected
by
leprosy
(26
from
each
state);
6
LGA
leprosy
control
supervisors
(3
from
Anambra
and
3
from
Ebonyi)
on
the
basis
of
one
supervisor
per
selected
LGA
in
each
state;
4
officers
from
Leprosy
Control
Units
of
Ministry
of
Health
in
the
two
states
(2
from
each
state)
and
one
official
each
from
Donor
Agency
supporting
leprosy
control
and
World
Health
Organization.
The
cluster
(multistage)
sampling
approach
involving
division
of
the
population
or
geographical
area
into
units
and
selecting
specific
number
of
these
units
by
simple
random
sampling
techniques
was
adopted
for
selection
of
members
of
the
public.
Table
2:
Local
Government
Areas
(LGA),
Communities
and
Villages
used
in
the
study
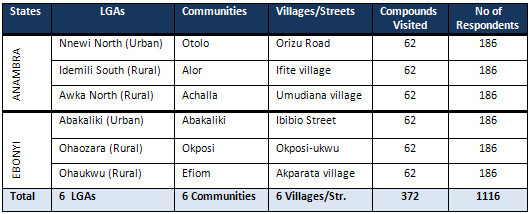 Source:
Field
Survey,
2010
Source:
Field
Survey,
2010
.
Three
instruments
were
combined
in
the
study
for
optimum
results.
Quantitative
data
were
collected
through
questionnaire
with
closed
and
open
ended
items
administered
on
a
one-on-one
(other
administered)
basis
with
all
respondents.
The
instrument
was
pre-tested
by
the
researcher
and
five
Field
Assistants
pre-trained
for
the
purpose
in
four
sessions
outside
the
study
communities,
at
Eziani-
Ihiala,
in
Ihiala
LGA
of
Anambra
state
with
40
compounds/
households
and
120
respondents.
This
was
to
ensure
reliability
and
suitability
of
the
instrument
to
meet
study
objectives.
The
language
of
administration
was
Igbo,
spoken
in
the
area,
because
there
were
many
respondents
who
could
not
read,
write
or
understand
English
language.
Nonetheless,
English
was
used
where
any
respondent
showed
preference
for
English
language.
The
instrument
which
was
originally
in
English
was
translated
into
the
local
language,
which
is
Igbo
and
retranslated
into
English,
to
provide
both
Igbo
and
English
versions.
Same
sex
administration
of
questionnaire
was
carried
out
to
prevent
any
cultural
barriers
and
permit
free
discussion
or
responses
to
questionnaire
items.
Qualitative
data
were
gathered
through
Focus
Group
Discussions
(FGD)
and
In-Depth
Interview
(IDI).
The
FGD
involved
persons
affected
by
leprosy
(patients)
who
were
not
respondents
in
the
questionnaire
study.
There
were
four
FGD
sessions
with
6-12
participants
per
session.
Participants
were
segmented
along
gender.
Two
FGD
sessions
were
conducted
at
Mile
Four
Hospital
Abakaliki,
Ebonyi
state
for
male
and
female
groups
respectively.
The
other
two
were
conducted
at
Fr
Damian
Tuberculosis
and
Leprosy
Referral
Hospital
Nnewi,
Anambra
state.
Both
institutions
were
convenient
to
both
in
and
out-
patients.
Each
session
was
held
on
leprosy
clinic
days
which
are
usually
market
free
days
in
the
area
of
study.
The
moderator
of
the
FGD
was
of
the
same
sex
with
their
FGD
group
and
worked
with
the
co-operation
of
leprosy
control
staff
on
duty.
There
were
also
two
assistants
for
each
FGD
session.
The
language
of
administration
was
Igbo.
A
tape
recorder
and
field
notebook
was
used
to
record
proceedings.
One
assistant
took
notes
in
the
course
of
each
session
while
the
other
served
as
Tape
Recorder
Operator.
The
second
qualitative
tool
was
the
conduct
of
In-Depth
Interview
(IDI).
It
was
used
to
interrogate
four
officials
who
are
major
stakeholders
in
leprosy
control
project.
These
were
Leprosy
Control
Officers
or
their
assistant
in
the
two
states,
Medical
Officer
of
German
Leprosy
Relief
Association,
and
W.H.O's
Principal
Officer
for
Leprosy
Control
for
Southeast
Area
of
Nigeria.
The
interview
schedule
was
unstructured
and
tailored
to
generate
detailed
information
on
the
subject
of
study.
The
in-
depth
interviews
were
conducted
by
the
researcher
and
two
of
the
assistants
at
the
offices
of
the
stated
officials.
Tape
recorder
and
field
note
book
were
used
to
record
responses
from
interviewees.
The
interview
schedule
guided
the
interview
which
was
conducted
in
English
language
due
to
respondents'
preference
and
literacy
level.
Quantitative
data
gathered
in
the
course
of
research
were
analysed
with
the
help
of
the
Statistical
Package
for
the
Social
Sciences
(SPSS)
software.
Descriptive
statistics
like
frequency
distribution
tables,
mean,
median,
percentages
and
bar-charts
were
used
to
interpret
data.
One
correlation
analysis
(the
chi-square)
was
employed
in
hypotheses
test.
On
the
other
hand,
qualitative
data
generated
through
FGD
and
IDI
were
transcribed
and
organised
under
different
aspects
of
the
discussion
and
used
to
explain
quantitative
data
where
applicable.
One
thousand,
one
hundred
and
sixteen
(1116)
questionnaires
were
administered
out
of
which
1104
were
used
for
analysis
after
coding
and
cleaning/
editing
all
validly
completed
and
returned
questionnaire
schedules.
Results
and
their
analysis
were
presented
according
to
research
questions
for
easy
comprehension.
(a)
Socio-Demographic/Personal
Characteristics
of
Respondents
The
socio-demographic
profile
of
respondents
is
presented
in
Table
3
below.
Table
3:
Distribution
of
Respondents
by
Socio-Demographic
Characteristics
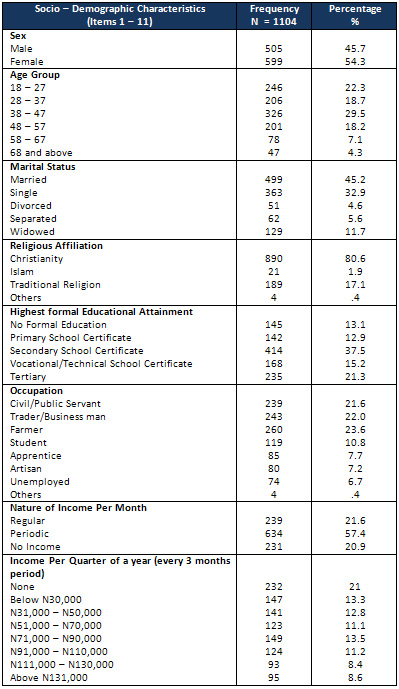
Source:
Field
Survey,
2010.
Table
3
shows
that
females
constituted
54.3%
of
the
total
respondents,
while
the
males
constituted
45.7%.
Many
of
the
respondents
(29.5%)
fall
within
the
age
bracket
of
38
-
47
years.
The
least
number
of
respondents
(4.3%)
came
from
the
age
-
group
of
45
years
and
above.
However,
the
modal
and
median
ages
were
41
and
45
years
respectively.
Also,
the
mean
age
of
respondents
was
40.33
years
with
a
standard
deviation
of
13.45.
With
regard
to
the
marital
status
of
the
respondents,
45.2%
were
married
while
32.9%
are
single.
The
widowed,
separated
and
divorced
respondents
were
very
few
(11.7%,
5.6%
and
4.6%
respectively).
The
large
number
of
married
respondents
illuminates
the
high
premium
placed
on
marriage
and
family
institution
in
the
area.
Similarly,
divorce
is
low
probably
because
the
value
system
abhors
it.
Being
married
and
having
stable
marriage
are
accorded
high
esteem
and
social
honour
among
Igbo
people.
With
respect
to
religious
affiliation,
the
table
clearly
shows
that
more
than
three-quarters
of
the
respondents
(80.6%)
were
Christians.
A
few
of
the
respondents
belong
to
other
religious
groups
including
Islam
(1.9%),
traditional
religion
(17.1%)
and
other
unspecified
groups
(.4%).
In
terms
of
highest
formal
educational
attainment,
those
who
possess
secondary
school
certificate
constituted
37.5%
of
the
respondents.
Other
categories
of
educational
attainment/
certification
were
tertiary
(21.3%),
vocational/technical
school
(15.2%),
and
primary
school
certificate
holders
(12.9%).
With
only
13.1%
of
the
respondents
without
any
form
of
formal
education,
the
literacy
level
in
the
area
is
relatively
high.
However,
more
respondents
from
Anambra
state
(27.7%)
had
tertiary
education
than
those
from
Ebonyi
state
where
only
15%
had
tertiary
education.
The
respondents
were
almost
equally
divided
across
three
major
occupations.
These
are
farmers
(23.6%),
traders
(22%),
and
civil/public
servants
(21.6%).
Students,
apprentices,
artisans
and
the
unemployed
were
few.
They
constituted
10.8%,
7.7%,
7.2%,
and
6.7%
respectively.
The
occupational
distribution
of
the
respondents
highlighted
above
mirrors
the
popular
description
of
Ebonyi
state
as
food
basket
(major
agricultural
zone)
of
the
nation,
and
Anambra
state
as
center
for
commerce
and
other
entrepreneurial
activities.
The
predominance
of
farmers
and
traders
in
the
area
of
study
is
therefore
not
a
major
surprise.
However,
the
nature
of
income
reveals
that
most
of
the
respondents
(57.4%)
earn
periodic
income;
21.6%
earn
regular
income
on
monthly
basis,
while
20.9%
earn
no
income
at
all.
In
terms
of
actual
income
earned
per
quarter
(every
three
months),
many
of
the
respondents
(21%)
earn
no
income.
These
include
students,
apprentices,
some
artisans
and
the
unemployed.
More
than
two-thirds
of
these
respondents
that
earn
no
income
are
from
Anambra
state.
Furthermore,
13.5%
of
the
respondents
earn
below
N30,000
per
quarter,
and
only
8.6%
earn
above
N131,000
per
quarter.
This
shows
that
income
status
of
individuals
within
the
area
of
study
is
generally
low.
The
mean
income
per
quarter
of
the
respondents
is
about
N59,033
with
a
standard
deviation
of
N45,933.
The
median
income
stood
at
about
N55,378.
(c)
Research
Question
1:
What
types
of
social
and
economic
rehabilitation
programmes
are
available
to
persons
affected
by
leprosy
in
Anambra
and
Ebonyi
states?
Data
relevant
to
the
research
question
are
presented
in
Tables
4
and
5
below.
Table
4:
Distribution
of
Respondents
by
their
opinion
on
whether
Social
and
Economic
Rehabilitation
is
a
component
of
Leprosy
Control
in
their
Area.
Source:
Field
Survey,
2010.
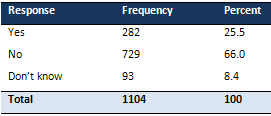
Table
4
shows
that
66%
of
the
respondents
stated
that
there
was
no
SER
component
of
leprosy
control
in
their
area.
Only
25.5%
of
the
respondents
acknowledged
existence
of
any
form
of
SER
activities.
However,
more
respondents
from
Ebonyi
state
(75.3%)
were
of
the
view
that
SER
was
not
a
component
of
leprosy
control
in
their
state
as
against
56.6%
who
had
a
similar
opinion
at
Anambra
state.
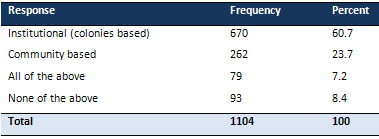
Also,
most
of
the
respondents
(60.7%)
identified
the
core
rehabilitation
strategy
as
institutional
or
colony
based
(see
Table
5
below).
This
suggests
that
the
current
thrust
of
World
Health
Organization
(WHO)
towards
Community
Based
Rehabilitation
(CBR)
is
yet
to
make
an
appreciable
impact
in
the
two
states.
Table
5:
Distribution
of
Respondents
by
their
opinion
on
Rehabilitation
Strategy
adopted
by
Leprosy
Control
Programme
Source:
Field
Survey,
2010.
The
specific
SER
activities
provided
or
available
to
patients
were
also
identified.
They
included
resettlement
of
persons
affected
by
leprosy
in
colonies
which
ranked
tops
with
36.7%
of
responses.
Others
were
public
re-orientation
(17.3%),
vocational
/
occupational
training
(12.6%),
and
financial
support
to
set-up
small
businesses
(10.9%).
Furthermore,
approximately
half
of
the
respondents
(49.5%)
were
of
the
view
that
government,
NGOs,
companies,
philanthropists
and
faith
based
organizations
do
not
provide
support
for
SER
activities.
Only
about
14.9%
and
11.1%
of
the
respondents
acknowledged
NGO
and
government
support
for
SER
activities
as
part
of
leprosy.
Similarly,
most
of
the
respondents
(79.0%)
were
also
of
the
opinion
that
vocational
training
was
not
provided
to
leprosy
patients.
In
a
similar
vein,
most
of
the
respondents
(78.8%)
submitted
that
vocational
training
in
the
areas
of
carpentry;
shoe
making,
tailoring,
weaving
and
soap
making
were
not
provided
as
part
of
leprosy
control.
Many
of
the
respondents
(68.4%)
equally
stated
that
there
were
no
community
based
supportive
activities
aimed
at
rehabilitation
of
patients
and
stigma
reduction.
These
responses
reveal
the
lapses
of
the
control
programme
in
the
two
states
in
the
area
of
SER
of
persons
affected
by
leprosy.
The
high
negative
responses
to
SER
variables
were
however
not
fully
corroborated
by
IDI
participants.
More
than
half
of
the
IDI
participants,
particularly
health
workers
enumerated
efforts
at
rehabilitation
of
patients
but
accepted
that
a
lot
still
needs
to
be
done.
An
IDI
respondent
from
Anambra
state
reported
thus-
There
is
a
Community
Based
Rehabilitation
(CBR)
Committee
in
Anambra
state.
The
German
Leprosy
Relief
Association
(GLRA)
pays
about
12
persons
affected
by
leprosy
a
monthly
welfare
support
of
N2000.
Two
(2)
dependants
are
also
currently
benefiting
from
educational
support
from
GLRA.
The
respondent
also
recounted
that
financial
support
(loan)
to
the
tune
of
N10,000
for
trading
or
farming
was
provided
in
the
past
but
regretted
that
patients
did
not
repay
such
loans
to
enable
others
to
benefit.
On
their
part,
male
and
female
FGD
participants
at
Mile
4
Hospital
Abakaliki
recounted
promises
made
toward
their
social
and
economic
rehabilitation.
They
however
maintained
that
such
promises
are
yet
to
materialize.
Male
and
female
FGD
participants
at
Fr
Damian
TB
and
Leprosy
Hospital,
Nnewi/Amichi
in
Anambra
state
also
decried
the
absence
of
SER
programme
for
them.
They
maintained
that
they
depend
on
donations
of
people
of
goodwill
to
subsist.
(d)
Research
Question
2:
What
are
the
perceived
outcomes
of
social
and
economic
rehabilitation
of
persons
affected
by
leprosy
in
Anambra
and
Ebonyi
states?
Data
relevant
to
the
research
question
are
reflected
in
the
bar
chart
(Figure
2)
and
Table
6
below.
Figure
2:
Respondents
Assessment
of
Social
and
Economic
Rehabilitation
(SER)
Activities
of
Persons
Affected
by
Leprosy
in
their
Community
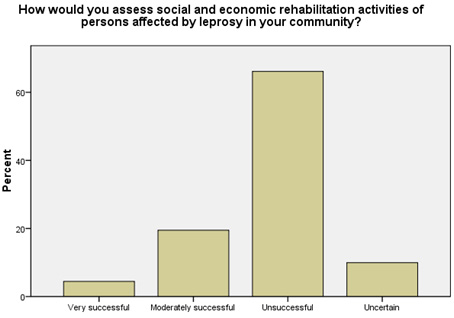
The
chart
above
shows
that
most
of
the
respondents
(66.1%)
assessed
SER
component
of
the
leprosy
control
programme
in
Anambra
and
Ebonyi
states
as
unsuccessful.
This
suggests
high
neglect
of
SER
activities
in
leprosy
control
in
the
area.
However,
more
respondents
from
Ebonyi
state
(88%)
subscribed
to
the
opinion
that
SER
was
unsuccessful
as
against
44.1%
from
Anambra
state
who
shared
similar
views.
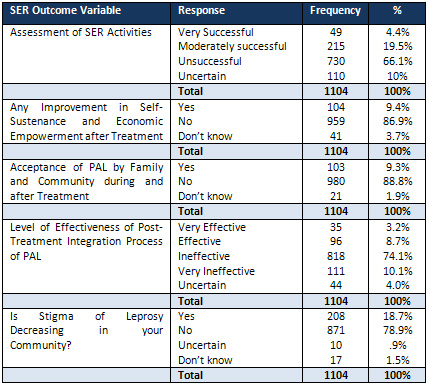
Table
6
below
summarizes
other
findings
on
perception
of
outcome
of
SER
activities.
Again,
the
table
shows
high
negative
responses
to
five
SER
outcome
variables
examined.
The
situation
points
to
the
magnitude
of
unmet
expectations
of
respondents
in
the
area
of
social
and
economic
rehabilitation
of
victims
of
leprosy.
Table
6:
Distribution
of
Respondents
by
their
Assessment
of
Outcomes
of
SER
Activities
in
Leprosy
Control
Source:
Field
Survey
2010.
The
FGD
results
agree
to
a
large
extent
with
the
above
table
over
poor
SER
outcomes.
The
opinion
of
a
female
FGD
participant
at
Fr
Damian
TB
and
Leprosy
Hospital,
Nnewi
summarizes
FGD
data
on
SER
outcome
in
both
states
is
as
follows
-'We
have
not
benefited
anything
except
free
drugs.
Others
are
but
promises.
I
look
forward
to
when
I
shall
not
be
called
all
sorts
of
names
and
be
truly
accepted
and
seen
as
a
human
being
in
my
community;
when
my
ulcer
and
deformed
fingers
are
disregarded
and
I
could
shop
with
money
earned
from
my
work
and
not
from
begging.
I
beg
out
of
frustration.
I
dislike
it'.
On
their
part,
many
IDI
participants
spoke
of
some
limited
level
of
success
in
SER
activities.
An
IDI
respondent
from
World
Health
Organization's
(WHO)
Zonal
Office
at
Enugu
clarified
as
follows-
'WHO
has
no
direct
SER
programme
for
persons
affected
by
leprosy.
However,
she
(WHO)
collaborates
with
partners
to
provide
cash
stipends,
vocational
training
and
prosthesis'.
The
respondent
however
noted
that
funding
for
SER
is
low,
and
that
SER
has
not
made
much
impact
in
leprosy
control
due
to
incomprehensive
data
base
on
patients'
needs.
Above
all,
the
respondent
lamented
that
many
leprosy
patients
were
already
disadvantaged
before
starting
treatment
and
SER
cannot
reverse
their
situation.
The
negative
perception
of
SER
outcome
cannot
be
totally
divorced
from
impediments
posed
by
limited
funds
and
poor
capacity
of
health
workers.
Late
commencement
of
treatment
and
its
associated
lifelong
disabilities
(present
even
after
completing
treatment)
cast
further
doubts
about
any
serious
plan
for
prevention
of
disabilities
(POD).
POD
which
is
a
key
component
of
SER
appears
to
be
weak
in
the
two
states.
In
the
context
of
weak
POD,
the
public
opinion
is
that
nothing
has
improved
as
long
as
disabilities
remain
with
patients.
The
situation
is
compounded
by
the
absence
of
corrective
surgery
facilities
for
persons
affected
by
leprosy
at
the
leprosy
clinics.
The
researcher
also
recognizes
that
weak
rehabilitation
plan
may
have
contributed
to
the
emergence
of
co-operatives
involving
persons
affected
by
leprosy
in
their
attempt
to
help
themselves.
More
than
two-thirds
of
the
respondents
(70.9%)
acknowledged
the
existence
of
such
co-operatives
which
serve
as
coping
mechanisms
to
life
challenges
posed
by
leprosy.
(d)
Research
Question
3:
How
do
people
of
Anambra
and
Ebonyi
States
of
Southeast
Nigeria
perceive
the
level
of
funding
for
social
and
economic
rehabilitation
of
persons
affected
by
leprosy
in
their
area
in
terms
of
its
adequacy?
Table
7:
Distribution
of
Respondents
according
to
State
of
Origin
and
their
Assessment
of
Level
of
Funding
for
Leprosy
Control
Programme
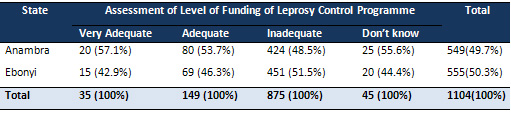
X2
=
2.883,
df
=
3,
p
=
.410
From
Table
7
it
could
be
seen
that
there
is
no
significant
difference
in
the
mode
of
assessment
/
perception
of
funding
for
leprosy
control
activities
across
the
two
states.
Almost
an
equal
number
of
respondents
from
both
states
saw
funding
for
leprosy
control
as
inadequate.
This
suggests
that
funding
problem
remains
a
common
handicap
to
leprosy
control
in
both
states.
From
the
analysis
of
field
data,
it
was
observed
that
leprosy
was
considered
a
serious
skin
related
health
problem
in
the
area
studied.
This
is
consistent
with
findings
in
a
previous
study
by
Nicholls
(2000).
The
medical
and
social
problems
associated
with
leprosy
have
also
been
well
documented
by
scholars
(see
Federal
Ministry
of
Health,
FMOH
1997;
Sofola
1999,
Ogbeiwi
2005,
Rafferty
2005
etc).
The
fact
that
there
was
very
poor
performance
of
social
and
economic
rehabilitation
(SER)
component
of
leprosy
control
in
the
two
states
was
a
major
finding.
This
area
is
certainly
the
weakest
aspect
of
leprosy
control
in
the
two
states.
Most
study
participants
responded
negatively
to
the
issue
of
availability
of
SER
activities
and
to
five
SER
outcome
variables
that
were
examined.
Such
poor
performance
of
SER
component
is
a
departure
from
the
submissions
of
both
Smith
(2000)
and
WHO
(1999).
They
have
held
that
SER
should
actually
be
a
priority
in
leprosy
control
projects.
The
respondents
in
this
study
were
of
the
opinion
that
vocational
training,
stigma
reduction,
economic
empowerment
and
acceptance
of
PAL
by
community
have
all
failed
to
materialize
as
envisaged.
The
finding
of
this
study
with
respect
to
SER
is
also
totally
at
variance
with
those
of
Nash
(2001)
who
held
that
SER
had
attained
significant
levels
of
success
in
Nigeria
or
that
patients
had
fitted
into
new
economic
roles
that
won
them
social
acceptance
and
respect.
The
disconnect
in
findings
between
the
present
study
and
that
of
Nash
(2001)
could
be
explained
by
the
time
lag
between
the
two
studies
and
the
fact
that
Nash
focused
on
Northern
Nigeria
while
the
present
study
was
located
at
the
Southeast
zone.
Above
all,
institutional
(colony
based)
rather
than
community
based
rehabilitation
strategies
were
still
being
practiced
with
limited
results.
Factors
accountable
for
the
deplorable
SER
status-quo
include
belief
systems,
low
public
enlightenment,
poor
logistics,
low
knowledge,
lack
of
funds,
inadequate
and
non-enthusiastic
health
staff.
There
was
also
no
strategy
in
place
to
ensure
that
rehabilitation
takes
on
a
multi-sectoral
approach
best
suited
for
its
operations.
The
situation
was
further
compounded
by
the
fact
that
the
Social
Welfare
Department
and
other
important
agencies
were,
in
the
opinion
of
respondents,
operating
at
a
distance
away
from
SER
activities
in
leprosy
control.
The
synergy
and
collaboration
that
ought
to
characterise
their
relationship
was
nonexistent.
These
observations
on
the
state
of
rehabilitation
of
PAL
in
Anambra
and
Ebonyi
states
could
be
accountable
for
the
conclusion
drawn
by
Nigeria
Television
Authority
(NTA,
2011)
to
the
effect
that
rehabilitation
of
persons
affected
by
leprosy
is
largely
unaddressed
in
Nigeria.
The
role
of
funding
in
leprosy
control
has
been
strongly
emphasized
by
Anyam
(2001)
and
Osakwe
(2004).
This
study
affirmed
their
contentions
but
also
revealed
that
most
respondents
actually
saw
the
level
of
funding
for
leprosy
control
in
Anambra
and
Ebonyi
states,
especially
as
applicable
to
SER,
as
inadequate.
Many
IDI
respondents
(health
workers)
reported
poor
budgetary
allocation
to
leprosy
control.
Also,
leprosy
patients
who
were
participants
in
the
FGD
sessions
recounted
severe
financial
difficulties
which
they
experienced.
These
observations
justify
the
position
of
the
political
economy
framework
that
government
often
channel
resources
to
maintenance
of
production
to
the
neglect
of
core
social
goal
of
securing
and
improving
health.
A
properly
funded
leprosy
control
programme
will
be
responsive
to
both
medical
and
economic
needs
of
patients.
| CONCLUSIONS
AND
RECOMMENDATIONS
|
Based
on
the
findings
from
the
present
study,
the
following
recommendations
can
be
made:
1.
There
is
immense
need
to
improve
the
level
of
community
involvement,
ownership
and
participation
in
the
programme
which
is
currently
very
low.
The
involvement
of
community
leaders
is
a
laudable
step
in
this
direction.
In
addition,
the
role
of
social
groups
like
age-grades,
women
groups,
clubs
and
faith-based
associations
will
positively
affect
decisions
toward
ameliorating
the
effects
of
socio-cultural
factors
on
leprosy
control
programme.
With
the
support
and
participation
of
the
community,
socio-cultural
practices
and
beliefs
that
negatively
affect
leprosy
control
should
be
abolished
/prohibited.
2.
There
is
need
for
a
holistic
leprosy
control
programme
which
should
include
crucial
components
like
social
and
economic
rehabilitation
and
reintegration
of
persons
affected
by
leprosy
into
their
communities.
Such
a
holistic
package
will
ensure
that
persons
affected
by
leprosy
are
properly
treated.
It
will
also
ensure
that
they
are
economically
empowered
and
remained
socio-politically
relevant
despite
their
disease
experience.
3.
Existing
legislations
should
be
enforced
and
new
ones
enacted
to
adequately
protect
persons
affected
by
leprosy
from
all
forms
of
stigmatization,
discrimination,
and
violations
of
their
fundamental
human
rights.
Such
measure
of
protection
will
encourage
them
to
live
normal
lives
devoid
of
social
seclusion
or
withdrawal
and
to
positively
respond
to
their
problem.
4.
There
is
immense
need
for
inter-agency
collaboration
to
meet
the
goals
of
leprosy
control.
The
programme
should
liaise
with
National
Poverty
Alleviation/
Eradication
Programme
and
the
Social
Welfare
Department
etc
to
address
issues
of
poverty,
welfare
and
social
integration
as
they
affect
leprosy
patients.
The
Ministry
of
Education
at
the
three
tiers
of
government
should
also
be
involved
with
a
view
to
including
leprosy
as
a
subject
of
study
in
the
curricula
of
schools.
This
is
sequel
to
the
finding
that
formal
education
generally
has
positive
impact
on
leprosy
control.
5.
Government
at
all
levels
should
demonstrate
strong
political
will
and
commitment
toward
leprosy
control.
This
should
be
done
through
adequate
funding,
prompt
release
of
budgeted
sums,
provision
of
infrastructure,
logistics,
training
and
motivation
of
leprosy
control
staff
through
prompt
payment
of
entitlement
and
allowances.
6.
There
should
also
be
a
synergy
between
donor
agencies,
non-governmental
organizations,
development
partners
and
government
departments
involved
in
leprosy
control.
All
channels
of
energy
leakage,
wasteful
duplication
of
functions
and
confrontations
should
be
blocked.
7.
Because
of
observed
negative
impact
of
socio-cultural
factors
like
belief
system
on
leprosy
control,
there
is
immense
need
to
enhance
the
capacity
of
health
workers
to
understand
socio-cultural
factors
related
to
leprosy.
This
could
be
achieved
through
on
the
job
training
to
equip
them
about
behaviour
change
techniques.
Furthermore,
social
scientists
that
are
likely
to
better
understand
and
plan
interventions
against
such
socio-cultural
dimensions
should
be
part
of
leprosy
control
teams
in
the
spirit
of
inter-disciplinary
co-operation
and
better
results.
Adagba
.K.
(2011).
Interview
Granted
to
Nigerian
Television
Authority
(NTA)
to
mark
50
years
of
Tackling
Leprosy
Problem
in
Nigeria,
NTA
Weekend
File,
5th
February.
Bryceson,
A.
&
Pfaltzgraff,
R.E.
(1990).
Leprosy.
United
Kingdom:
Longman
Group
UK
Limited.
Chukwu,
J.N.
(2004,
April).
Towards
a
Leprosy
free
Society:
The
Role
of
Tuberculosis
and
Leprosy
Supervisors
(TBLS).
Being
an
Address
Presented
at
the
Quarterly
Meeting
of
Anambra
State
Tuberculosis
and
Leprosy
Supervisors
Held
at
Local
Government
Hall,
Amawbia,
5th
-
7th.
Doyal,
L.
(I979).
The
Political
Economy
of
Health.
London:
Pluto
Press.
Durkheim,
E.
(1938).
The
Rules
of
Sociological
Method.
Glencoe:
Free
Press.
Eboh,
W.
(1999).
Leprosy
Control
in
Nigeria:
Past,
Present
and
Future,
TBL
Magazine
and
Photo
Album.
Zaria:
Batch
21
TBLS
Trainees.
Ekiti,
P.
(2010).
Address
to
mark
'2010
World
Leprosy
Day
on
theme
-
Justice:
Fighting
a
just
course'
World
Health
Organization,
Nigeria.
Erinosho,
O.A.
(2006).
Health
Sociology.
Ijebu
Ode:
Bulwark
Consult.
Ezekpeazu,
J.I.
(2000).
Leprosy:
Causative
Organism,
Mode
of
Spread,
Signs
and
Symptoms,
Diagnosis,
Differential
Diagnosis,
Classification
and
Treatment.
Paper
Presented
at
World
Leprosy
Day
Conference
Held
at
Madonna
University,
Okija,
9th
-
11th
Feb.
Federal
Ministry
of
Health,
Department
of
Primary
Health
Care
(1997).
National
Tuberculosis
and
Leprosy
Control
Programme
(NTBLCP),
Workers'
Manual,
2nd
Edition.
Federal
Ministry
of
Health,
Department
of
Public
Health
(2004).
National
Tuberculosis
and
Leprosy
Control
Programme
(NTBLCP)
Workers'
Manual,
4th
Edition.
Grand,
A.L.
(1997).
Women
and
Leprosy:
A
Review.
Leprosy
Review,
68,
203
-
211.
Hahn,
R.A.
(1999).
Anthropology
in
Public
Health:
New
York:
Oxford
University
Press.
Haralambos,
M.,
Holborn,
M.
&
Heald,
R.
(2004).
Sociology:
Themes
and
Perspectives.
London:
Harper
Collins
Publishers.
http://en.wikipedia.org/wiki/phenomenologicalsociology
Retrieved
15th
May,
2009.
Ifemesia,
C.
(1979).
Traditional
Humane
Living
among
the
Igbo:
An
Historical
Perspective.
Enugu:
Fourth
Dimension
Pub.
Co.
Ltd.
Kaufmaun,
A.,
Neville,
J.
&
Mariam,
S.G.
(1993).
The
Social
Dimension
of
Leprosy.
London:
TALMILEP
Kaur,
H.,
&
Ramesh,
V.
(1994).
Social
Problems
of
Women
Leprosy
Patients:
A
Study
at
Two
Urban
Leprosy
Centres
in
Delhi.
Leprosy
Review,
65,
361
-
375.
Khulmann,
E.
(2009).
From
Women's
Health
to
Gender
Mainstreaming
and
Back
Again:
Linking
Feminist
Agencies
and
New
Governance
in
Healthcare.
Current
Sociology,
57(2),
Monograph
1,
135
-
154.
Lemert,
E.M.
(1951).
Social
Pathology.
New
York:
McGraw
Hill
Book
Co.
Lockwood,
D.
(2000).
Consequences
of
Leprosy
and
Socio-Economic
Rehabilitation.
Leprosy
Review,
71(4),
417
-
419.
Macaden,
V.P.
(1996).
An
Introduction
to
Community
Based
Rehabilitation
in
Leprosy.
Partners
Magazine
for
Paramedical
Workers.
1
(30),
3
-
5.
Mgbenwelu,
L.
(1999).
An
Opening
Address
on
the
Occasion
of
the
Training
of
Health
Workers
on
Leprosy
Care
at
Ihiala
Local
Government,
15th
October.
Naidoo,
J.,
&
Wills,
J.,
(2001).
Health
Studies:
An
Introduction.
New
York:
Palgrave
Publishers.
Nash,
J.
(2001).
What
is
Rehabilitation.
Partners
Magazine
for
Paramedical
Workers
in
Leprosy,
1
(38),
3-7
National
Population
Commission
(2006).
2006
Population
and
Housing
Census
of
the
Federal
Republic
of
Nigeria.
National
and
State
Population
and
Housing
Tables
(Priority
Tables
Vol.1)
Navara,
V.
(1979).
Medicine
under
Capitalism.
London:
Crown
Helm.
Nicholls,
P.G.
(2000).Guidelines
for
Social
and
Economic
Rehabilitation.
Leprosy
Review,
71,
422
-
465.
Nigeria
Television
Authority
(2011).50
years
of
Tackling
Leprosy
Problem
in
Nigeria,
NTA
Weekend
File'
5th
Feb.
Nwala,
T.U.
(1985).
Igbo
Philosophy.
Lagos:
Literame
Publishers
Ltd.
Nwankwo,
I.U
(2010).Alienation
and
Suicidal
Tendencies
among
Leprosy
Patients
Anambra
State.
Practicum
Psychologia,
2(2),
40-48.
Nwankwo,
S.N.
(2006).
Compliance
Status
of
Multiple
Drug
Therapy
(MDT)
By
Leprosy
Patients
in
Imo
State
from
2000-2004.
Unpublished
Postgraduate
Diploma
Thesis,
Imo
State
University,
Nigeria.
Nwosu,
H.N.
(2002).
Politics
and
Administration
of
Igbo
Traditional
Society.
In
Ofomata,
G.E.K.
(Ed.).
Survey
of
the
Igbo
Nation.
Onitsha:
Africana
First
Publishers
Ltd.
Ogbeiwi,
O.I.
(2005).
Progress
towards
the
Elimination
of
Leprosy
in
Nigeria:
A
Review
of
the
Role
of
Policy
Implementation
and
Operational
Factors.
Leprosy
Review,
76(1),
65
-
76.
Ogoegbulem,
S.A.
(2000,
February).
Forging
New
Partnerships
for
Effective
Leprosy
Control.
Paper
Presented
at
a
Three
Day
National
Workshop
to
Commemorate
World
Leprosy
Day,
Held
at
Madonna
University
Okija,
9th
-
11th
.
Olisa,
M.S.O.
(2002).
Igbo
Traditional
Socio-Political
System.
In
Ofomata,
G.E.K.
(Ed).
A
Survey
of
the
Igbo
Nation.
Onitsha.
Africana
First
Publishers
Ltd.
Onokala,
P.C.
(2002).
Trade
and
Transport.
In
Ofomata,
G.E.K(ed).
A
Survey
of
the
Igbo
Nation.
Onitsha:
Africana
First
Publishers
Ltd.
Osakwe,C.
(2004,
April).
Pre-requisites
for
an
Effective
Tuberculosis
and
Leprosy
Control
Programme.
An
Address
Presented
at
the
Quarterly
Meeting
of
Anambra
State
Tuberculosis
and
Leprosy
Supervisors
Held
at
Local
Government
Hall,
Amawbia.
5th
-
7th.
Pearson,
J.M.H
(1988).
Essentials
of
Leprosy.
India:
German
Leprosy
Association
and
TALMILEP.
Rafferty,
J.
(2005).
Curing
the
Stigma
of
Leprosy.
Leprosy
Review,
76(2),
119
-
126.
Rao,
.S.,
Garole,
.V.
&
Walawalker,
.S.
(1996).
Gender
Differentials
in
the
Social
Impact
of
Leprosy.
Leprosy
Review,
67,
190-199.
Ridley,
D.S.,
&
Jopling,
W.H.,
(1966).
Classification
of
Leprosy
According
to
Immunity.
International
Journal
of
Leprosy,
34,
255
-
273.
Robinson,
.I.
(1990).
Personal
Narratives,
Social
Careers
and
Medical
Courses.
Social
Science
and
Medicine,
1173
-
1186.
Schaefer,
R.T.,
&
Lamm,
R.P.
(1997).
Sociology:
A
Brief
Introduction.
USA:
The
Mc
Graw-Hill
Companies
Inc.
Scott,
J.
(2000).
The
Psychosocial
Needs
of
Leprosy
Patients.
Leprosy
Review,
71(4),
486
-
491.
Shlomo,
A.
(1968).
Socio-Political
Thought
of
Karl
Marx.
London:
Cambridge
University
Press.
Srivinasan,
H.
(1999).
The
Problem
and
Challenge
of
Disability
and
Rehabilitation
in
Leprosy.
Article
retrieved
April
20,
2009
from
http://www.cefpas.it/leprosy/disabilities/Doc
Rehabilitation.htm
Smith,
C.
(2000).
Leprosy
after
the
Year
2000.
Partners
Magazine
for
Paramedical
Workers,
1(37),
3-6.
Sofola,
O.
(1999).
Leprosy
Elimination
Campaigns:
The
Nigerian
Experience.
Leprosy
Review,
70,
465
-
471.
Turner,
J.H.
(1978).
The
Structure
of
Sociological
Theory.
Homewood
Illinois:
The
Dorsey
Press.
Uzozie,
L.C.
(2002).
Igbo
Concepts
and
Beliefs
about
Land.
Its
Classification
and
Tenurial
System.
In
Ofomata,
G.E.K.(Ed.).
A
Survey
of
the
Igbo
Nation.
Onitsha:
Africana
First
Publishers
Ltd.
Valsa,
A.
(1999).
Psychological
Aspects
in
Leprosy.
Partners
Magazine
for
Paramedical
Workers
in
Leprosy,
2(36),
14
-
16.
Valencia,
L.B.
(1989).
Social
Science
Research
on
Social
Dimensions
of
Leprosy:
Where
are
we
going
from
here?
International
Journal
of
Leprosy,
57,
847
-
863.
Warndorff,
D.K.
&
Warndorff,
J.A.
(1990).
Leprosy
Control
in
Zimbabwe.
From
a
Vertical
to
a
Horintal
Programme.
Leprosy
Review,
61,
183
-
187.
World
Health
Organization.
(1982).
Chemotherapy
of
Leprosy
for
Control
Programmes.
World
Health
Organization
Technical
Report
Series,
675.
Geneva:
World
Health
Organization.
World
Health
Organization.
(1985).
Epidemiology
of
Leprosy
in
Relation
to
Control.
World
Health
Organization
Technical
Report
Series,
716.
Geneva:
WHO.
World
Health
Organization.
(1988).A
Guide
to
Leprosy
Control
(2nd
Ed.).
Geneva:
World
Health
Organization.
World
Health
Organization.
(1999).
Elimination
of
Leprosy
Status
Report
(Draft).
Geneva:
World
Health
Organization.
World
Health
Organization.(2000).
Guide
to
Eliminate
Leprosy
as
a
Public
Health
Problem
(1st
Ed.).
Geneva:
World
Health
Organization.
World
Health
Organization.
(2002).
Integrating
Gender
Perspectives
in
the
Work
of
WHO.
Geneva:
World
Health
Organization.
World
Health
Organization.
(2008).
Weekly
Epidemiological
Record,
33,
293
-
300.
Retrieved
15th
December,
2008
from
http://www.who.int/wer
World
Health
Organization.
(2010).
New
Case
Detection
and
Prevalence,
2005
-
2008
for
South-east
Zone
of
Nigeria.
WHO
South-east
Zonal
Office
Enugu.
Yawalker,
S.
J.
(1994).
Leprosy
for
Practioners
(5th
ed.).
Bombai:
Popular
Prakashan.
|

