|
The effectiveness of
life skills training on happiness, mental health,
and marital satisfaction in wives of Iran-Iraq
war veterans
Kamal Solati
Associate Professor, Department of Psychiatry,
Social Determinants of Health Research Center,
Shahrekord University of Medical Sciences,
Shahrekord, Iran
Correspondence:
Department of Psychiatry,
Shahrekord University of Medical Sciences, Rahmatiyeh,
Shahrekord, Iran,
Tel.: +98-3833338891,
Email: kamal_solati@yahoo.com
|
Abstract
Background:
Injury due to war or accidents causes
numerous mental, physical, and social
adverse effects on affected individuals
and their family.
Aims: This
study was conducted to determine the effectiveness
of life skills training on happiness,
mental health, and marital satisfaction
in wives of Iran-Iraq war veterans.
Methods and
Material: In this semi experimental,
controlled study with pretest-posttest,
102 veterans in Shahrekord, southwest
Iran were randomly assigned to two groups,
intervention and control, after they filled
out a written consent form. The intervention
group alone received training on four
domains of life skills, coping with stress,
problem solving, decision-making, and
communication skills, for eight weeks.
Oxford Happiness Questionnaire, General
Health Questionnaire (GHQ-28), and ENRICH
Marital Satisfaction Scale were administered
at three steps, before intervention, immediately
after intervention, and six months after
intervention (as follow-up). The data
were analyzed by analysis of covariance
in SPSS 23.
Results:
The mean scores of happiness and mental
health indicated a significant difference
between the two groups at posttest (P<001).
But in follow-up, the difference was significant
for neither of the variables (P>0.05).
Mean scores of marital satisfaction exhibited
significant difference at both posttest
(P<001) and follow-up (P=0.001) between
the two groups.
Conclusion:
Life skills training for veterans’
wives can help them promote their mental,
physical health, and marital satisfaction,
but the findings on follow-up indicate
that this effect is not lasting. Therefore,
life skills training should be done continuously
particularly to promote mental health
and happiness.
Key words: Mental
Health, Happiness, Life, War veterans
|
World Health Organization (WHO), with UNICEF
coordination, has launched Life Skills Training
Program as a primary prevention and comprehensive
project of health promotion in children and
adolescents. WHO defines life skills as “the
ability to behave adaptively and positively
to be capable of coping with life necessities
and challenges”. Furthermore, WHO has introduced
ten skills as main life skills including decision-making,
problem solving, creative thinking, critical
thinking, effective communication skills, interpersonal
relationships skills, self-awareness, empathy,
and coping with stress and emotions (1). Chronic
diseases can cause negative effects on quality
of life and various aspects of health (2-9).
Making attempts to understand and assist the
psychiatric victims of wars and accidents requires
psychiatric and psychological interventions
to promote and maintain their health (10). Studies
have shown that posttraumatic stress disorder
(PTSD) affects not only the patients but also
their family function such as family cohesion,
parents’ satisfaction, relationship with
spouse, spouse self-identification, and children’s
emotional and functional safety (11-14). The
veterans of Iran-Iraq War suffer from different
complications and trauma, decrease in libido,
offensive disorder, conflict, and psychotic
symptoms (15, 16) which can influence the happiness,
mental health, and marital satisfaction in them
and their families.
Happiness is a kind of feeling positive. Happiness
means increase in positive feelings, high life
satisfaction, and relief of negative feelings
(17). Experiences of happiness depend on self-concept.
People with low self-esteem and self-worth are
often unhappy (18). Happiness rate is likely
to increase through training in the ten life
skills.
Mental health is a state of well-being in which
people realize their potential, cope with routine
life stresses, can function usefully and efficiently,
and help community (WHO, 2005), and marital
satisfaction refers to individual experiences
of marriage that are only measured by response
to the degree of the pleasure derived from marriage
(19). Studies have indicated that dissatisfaction
with married life is associated with development
of depression (20, 21), and marriage compatibility
is lower in the wives of the veterans with PTSD.
Moreover, marriage compatibility was considerably
lower in the couples both with PTSD than those
with only the veteran suffering from PTSD (22).
A study has shown that the chemical veterans
of the Iran-Iraq War are dependent on others,
particularly their wives, and cannot do even
their daily activities and hence are under stress
(23).
Many studies have been conducted on the effect
of life skills training on different populations
with different problems indicating the efficiency
of this method. The effect of life skills training
on relief of stress, prevention of high risk
sexual behaviors, and abuse of alcohol and substances
in adolescents has been reported (24-27). Codony
et al found that life skills training for adolescents
caused increase in self-confidence, life satisfaction,
and improvement of problem solving (28). In
a study in Mexico, life skills training for
girls led to increased self-efficacy and self-esteem
after training (29).
The soldiers with PTSD have been reported to
be involved in family aggression more frequently
than those without PTSD (30). The studies have
shown that the families of the war-afflicted
people suffer from many problems requiring therapeutic
interventions. Accordingly, a significant decrease
in severe psychiatric disorders was seen in
the war-afflicted families following psychological
training (31).
The studies of the people injured due to war
or trauma (psychiatric and physical injuries)
and their families have indicated that it causes
not only psychological, physical, and social
impacts on the injured people but also affects
their family members, particularly wives, indirectly,
and is associated with many adverse effects
in different domains, including marital, family,
and interpersonal, as well as psychiatric disorders,
depression, and anxiety. Previous studies have
mainly described the problems in these families
and less frequently investigated the educative
and therapeutic interventions.
The training on managing anger and stress,
decision making, problem solving, and communication
skills delivered to the relatives of this subpopulation
of the community is likely to contribute to
both prevention and resolution of the current
problems.
Therefore, the present study was conducted
to investigate and follow up the effect of life
skills training on happiness, mental health,
and marital satisfaction in the veterans’
wives in southwest Iran. The findings of this
study can help plan for mental health promotion
in the veterans’ wives to resolve the marital
and familial problems and increase the rate
of life satisfaction in these families.
In this controlled, quasi-experimental study
with pretest and posttest, the study population
consisted of the wives of all veterans with
25-70% physical and psychiatric injuries due
to war in Shahrekord, southwest Iran. Sampling
was random and convenience. Because the participants
were selected from the Martyrs Foundation, primary
sampling was convenience. Then, as the list
of veterans with 25-70% injuries was provided,
102 veterans were selected according to convenience
sampling and then their wives were enrolled
in the study. Regarding first type error=0.05,
power=0.80, happiness mean score of 13.20 in
a previous study (32), and 87.2 difference in
effect size (delta=2.87), 48 people were assigned
to each group. To further the rigor of the study
and deal with possible attrition, 51 people
were included in each group and totally 102
people were investigated. The participants were
randomly assigned to two 51- people groups,
case and control. The research protocol was
registered as 89-5-10 by the ethics committee
of the university.
The participants in the intervention group attended
eight sessions of life skills training on four
domains, stress management, problem solving,
decision making, and communication skills. The
control group underwent no treatment.
The protocol of life skills training
The intervention group received life skills
training on four domains consisting of stress
management, problem solving, decision making,
and communication skills within eight sessions,
and the control group underwent no intervention.
To increase the efficiency of training, the
intervention group was subdivided into three
groups of 17 each and the training was conducted
within one 2-hour session per week separately
for each subgroup.
In each of these sessions, a skill was discussed
and the homework, including special forms appropriate
for the session content, was developed prior
to that session and assigned to be done at home,
in addition to the assignments within sessions.
This training was conducted by a trained and
experienced clinical psychologist. At the beginning
of any session, the previous session was examined
and assessed and then the new subject was introduced.
The subjects for stress management were an introduction
to stress, positive and negative stress, stress
impacts and consequences (physiological, psychological,
and behavioural), different methods of coping
with the problems specific to the veterans’
families, and assigning homework.
For problem solving skill, the sessions included
introduction to problem, steps of problem solving,
the ways of gathering data to arrive at solutions,
detecting different solutions in coping with
life problems and adopting the best one, the
ways of clear thinking and problem solving in
critical conditions, regulation and control
and precision, reconciliation to resolve conflicts,
the effect of problem solving on solving the
daily problems of the veterans’ families,
and assigning homework.
For decision making skill, the sessions included
the introduction to decision making, the significance
of decision making in life, steps of decision
making, gathering data as much as possible in
decision making, decision making precisely based
on the situations, planning for life, acceptance
of decision making consequences, and assigning
homework.
For communication skills, the sessions included
the introduction to communication, definition
of communication and associated factors, the
process of establishing communication, being
a good listener and the required skills for
listening efficiently, verbal and nonverbal
communication (features), effective methods
of communicating with others, assertiveness,
understanding others’ feelings, respect
for others’ ideas, the methods of saying
no to insensible requests, and assigning homework.
The study was conducted at three steps, i.e.
pretest, posttest after two months of life skills
training, and follow-up (six months after the
last intervention). The two groups were assessed
at each step of the study by administration
of the research instruments. Follow-up was considered
to assess the stability of the training in the
intervention group.
Methods of data collection:
The data were gathered by three questionnaires
as follows:
1. Oxford Happiness Questionnaire
This questionnaire, developed by Argyle et al,
consists of 29 four-choice items. Each item
is aimed to judge the happiness level of respondents.
Argyle et al (1989) reported the reliability
of this questionnaire 0.90 by Cronbach’s
alpha and 0.78 by test-retest with a seven-week
interval (33). This questionnaire was translated
into Persian by Alipoor and Noorbala and its
reliability has been reported 0.98 by Cronbach’s
alpha, 0.92 by split-half reliability, and 0.79
by test-retest with a three-week interval. Furthermore,
the face validity of the questionnaire has already
been confirmed (34).
2. General Health Questionaire-28
This 28-item questionnaire investigates the
illness, medical diseases, and general and mental
health within the past month with minimal and
maximal score of 0 and 56, respectively. This
questionnaire was developed by Goldberg in 1972
and has been translated into 38 languages and
is being administered in 70 countries. Its subscales
are physical symptoms, anxiety symptoms and
sleep disorder, social functioning, and depression
symptoms. High reliability and reliability have
been reported for different versions of this
questionnaire (35-37). Williams et al in a study
in England reported the reliability of this
questionnaire as approximately 80% (37). Furthermore,
its reliability has been confirmed for an Iranian
population with Cronbach’s alpha 0.97 (38).
3. ENRICH Marital Satisfaction Scale:
The original version of this scale consists
of 115 items and 12 subscales. Given the large
number of the scale’s items and the participants’
tiredness, a shortened, 47-item version of the
original scale was developed. The subscales
of this scale were personality issues, marital
relationship, resolution of conflict, financial
management, leisure activities, sexual intercourse,
marriage and children, relatives and friends,
and religious orientation. The replies to the
scale’s items were scored by a five-point
Likert scale consisting of severely dissatisfied,
moderately dissatisfied, very satisfied, and
extraordinarily satisfied. The reliability and
validity of this Scale have already been confirmed
(39).
The demographic data of the participants (marital
status, education level, age, place of residence,
occupation, disability percentage of the veterans,
and disability type) were recorded in a separate
checklist. To study the association of happiness
in the veterans wives, the mean (SD) scores
of the two groups at three steps of the study
were compared and the effect of difference on
happiness was investigated in the intervention
group by analysis of covariance. The data were
analyzed by SPSSv23.
The
mean
age
of
the
participants
was
40.61±5.49
years.
97.06%
of
the
participants
had
at
least
elementary
education.
The
highest
frequency
of
education
level
was
obtained
for
guidance
education
completion.
63.7%
of
the
participants
were
living
in
cities
and
the
rest
in
villages.
90.2%
were
housewives
and
only
9.8%
were
employed
(mainly
civil
servants).
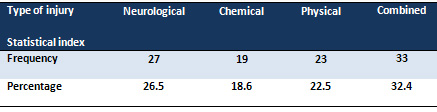
Regarding
the
types
of
veterans’
injuries,
26.5%
were
neurologically
injured,
18.6%
were
injured
by
chemical
weapons,
22.5%
were
physically
injured,
and
32.4%
had
combined
injury.
85%
of
the
veterans
were
25-40%
disabled
(Table
1).
Table
1:
The
types
of
the
injuries
of
participants’
spouses
Table
2
shows
both
frequency
and
percentage
of
injuries
of
the
participants’
spouses.
As
shown,
the
percentage
of
the
injuries
of
most
participants’
spouses
was
40%
and
the
percentage
of
the
least
number
of
participants’
injuries
was
45%-55%.
Click
here
for
Table
2:
The
frequency
and
percentage
of
injuries
of
the
participants’
spouses
The
mean
score
of
happiness
in
the
intervention
group
(49.39)
increased
more
markedly
than
the
control
group
(36.98)
at
follow-up
(Table
3).
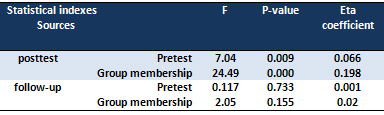
Furthermore,
Table
4
indicates
a
significant
difference
was
seen
in
happiness
mean
scores
between
the
two
groups
at
posttest
so
that
the
mean
difference
was
not
significant
after
controlling
for
pretest
scores
as
covariate.
Click
here
for
Table
3:
Statistical
indexes
of
crude
scores
of
happiness
in
participants
of
two
groups
Statistical
power
(0.998)
indicated
that
the
sample
size
was
adequately
large.
Therefore,
the
difference
between
the
two
groups
at
posttest
was
confirmed
and
life
skills
training
resulted
in
increased
happiness
in
the
veterans’
wives
at
posttest,
but
no
significant
difference
was
seen
in
the
mean
scores
of
happiness
between
the
two
groups
at
follow-up,
so
that
after
controlling
for
pretest
scores,
the
mean
difference
was
not
derived
as
significant
(Table
2).
Therefore,
life
skills
training
had
no
stable
effect
on
happiness
and
the
happiness
rate
decreased
over
time
in
the
participants.
Table
4:
Results
of
analysis
of
covariance
for
effect
of
life
skills
training
on
happiness
in
participants
at
posttest
and
follow-up
The
mean
score
of
mental
health
decreased
markedly
at
follow-up
in
the
intervention
group
(22.96).
This
means
that
after
life
skill
training,
mental
health
in
the
intervention
group
improved
but
did
not
change
in
the
control
group
(37.57)
(Table
5).
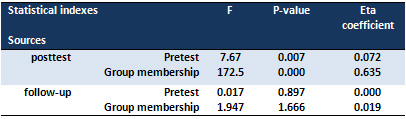
Table
6
indicates
that
there
is
a
significant
difference
in
the
mean
scores
of
mental
health
between
the
two
groups
at
posttest.
Eta
coefficient
(0.635)
indicated
that
63%
of
the
observed
difference
was
explained
by
life
skills
training.
Therefore,
life
skills
training
led
to
improvement
of
mental
health
in
the
veterans’
wives
at
posttest.
The
mean
scores
of
mental
health
were
not
significantly
different
between
the
two
groups
at
follow-up
(Table
7).
In
other
words,
life
skills
training
had
no
stable
effect
on
mental
health
in
the
veterans’
wives
and
the
mean
score
of
the
two
groups
was
approximately
equal
six
months
after
the
last
intervention.
Click
here
for
Table
5:
Statistical
indexes
of
crude
scores
of
mental
health
in
the
participants
of
two
groups
Table
6:
Results
of
analysis
of
covariance
for
effect
of
life
skills
training
on
mental
health
in
participants
at
posttest
and
follow-up
The
mean
scores
of
marital
satisfaction
in
the
intervention
group
at
pretest,
posttest,
and
follow-up
(135.68,
176.77,
and
159.20,
respectively)
increased
markedly
compared
to
the
control
group
(136.43,
141.05,
and
140.70,
respectively).
This
indicates
increase
in
marital
satisfaction
in
the
participants
(Table
7).
Click
here
for
Table
7:
Statistical
indexes
of
crude
scores
of
marital
satisfaction
in
the
participants
of
two
groups
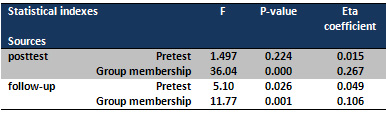
Table
8
indicates
that
a
significant
difference
is
seen
in
mean
score
of
marital
satisfaction
between
the
two
groups
at
posttest.
In
other
words,
life
skills
training
led
to
increased
marital
satisfaction
in
the
veterans’
wives
in
the
intervention
group
at
posttest
but
this
difference
was
not
notable
in
the
control
group.
Furthermore,
a
significant
difference
in
mean
score
of
marital
satisfaction
was
seen
between
the
two
groups
at
follow-up.
Therefore,
the
significant
difference
in
marital
satisfaction
between
the
two
groups
was
confirmed
at
follow-up,
and
life
skills
training
had
a
stable
effect
on
marital
satisfaction
in
the
veterans’
wives.
Table
8:
Results
of
analysis
of
covariance
for
effect
of
life
skills
training
on
marital
satisfaction
in
participants
at
posttest
and
follow-up
Obviously,
the
veterans’
families
are
affected
with
certain
psychological
and
marriage
incompatibility-associated
problems
and
therefore
their
quality
of
life
is
affected
(32).
Meanwhile,
veterans’
wives
are
likely
to
experience
greater
levels
of
stress
with
mental
health
and
life
satisfaction
being
at
higher
risk
than
other
family
members
(33).
These
findings
indicate
that
these
problems
have
many
negative
effects
on
the
veterans’
family
members
particularly
their
wives,
and
life
skills
training
can
greatly
enhance
the
methods
of
coping
with
these
problems
and
their
happiness.
The
present
study
indicated
that
the
life
skills
training
on
four
domains
of
coping
with
stress,
decision
making,
problem
solving,
and
interpersonal
and
social
relationships
could
result
in
the
relief
of
the
problems
in
these
families.
More
clearly,
life
skills
training
had
no
long-term
effect
on
happiness
in
the
veterans’
wives.
Carroll
et
al
study
demonstrated
that
training
life
skills
can
promote
coping
skills
in
the
families
of
military
staff
to
deal
with
adverse
and
unexpected
circumstances
(34).
Life
skills
training
like
mental
health
and
resilience
intervention
for
military
staff’s
wives
can
reduce
negative
mental
health
symptoms,
enhance
resiliency,
and
improve
coping
skills
(40).
Elliott
et
al’s
study
found
that
training
of
problem
solving
as
a
life
skill
was
effective
in
relieving
depression
in
the
family
caregivers
of
disabled
women
(41).
The
wives
of
war-afflicted
people
were
mainly
responsible
for
both
caring
for
the
veterans
and
the
related
problems
and
looking
after
children.
This
leads
to
heavy
psychological
and
physical
consequences
in
people
under
such
circumstances.
Therefore,
the
treatment
of
these
people
is
far
more
complex.
Naturally,
the
problems
in
these
families
are
much
more
complicated,
representing
that
they
require
continuous
training
to
cope
with
the
problems,
and
no
training
and
failure
to
support
them
leads
to
incidence
and
exacerbation
of
the
problems.
In
the
present
study,
life
skills
training
caused
promotion
of
mental
health
in
the
veterans’
wives.
Similarly,
Weines
et
al
indicated
that
psychological
education
of
Kosovo
War-afflicted
families
suffering
from
severe
psychiatric
disorders
led
to
remarkable
relief
of
symptoms
and
improvement
of
mental
health
(31).
Consistent
with
the
present
study,
Layne
et
al
reported
a
58%
decrease
in
PTSD
and
20%
decrease
in
depression
after
interventions
(42).
However,
in
the
present
study,
no
significant
difference
was
observed
in
the
mean
score
of
mental
health
between
the
two
groups
at
follow-up.
In
other
words,
life
skills
training
had
no
continuous
and
long-term
effect
in
treating
symptoms
and
promoting
mental
health
in
the
veterans’
wives,
which
is
partially
inconsistent
with
the
study
of
Layne
et
al
that
reported
an
81%
decrease
in
PTSD
symptoms
and
61%
decrease
in
depression
symptoms
four
months
after
the
last
intervention
(at
follow-up)
in
war-afflicted
adolescents
(42).
As
previously
argued,
this
inconsistency
could
be
due
to
differences
in
the
participants’
experiences.
The
results
of
marital
satisfaction
indicated
that
life
skills
training
led
to
a
stable
increase
in
marital
satisfaction
in
the
veterans’
wives.
The
findings
of
the
present
study
are
consistent
with
the
study
of
Hojjat
et
al
of
PTSD
effect
on
the
spouses
of
veterans
with
PTSD.
They
conclude
that
education
of
coping
with
stress
was
effective
in
increasing
the
marital
satisfaction
in
these
women
(43).
The
researchers
of
this
study
argued
that
the
symptoms
of
emotional
indifference
and
anger
should
be
especially
addressed
in
such
people
and
treatment
of
the
patients
with
PTSD
should
be
based
on
life
skills
training
and
support
for
family
(44).
The
present
study
can
demonstrate
that
the
families
of
military
staff
with
PTSD
suffer
from
some
problems
that
may
be
transferred
even
from
one
generation
to
another,
including
the
problems
related
to
intimacy
and
sociability,
marriage
incompatibility,
adaptive
communication
and
physical
aggressiveness,
disorders
of
interpersonal
skills,
and
marital
issues
(45-47).
The
life
skills
training
used
in
the
present
study
could
relieve
the
above
problems
and
strengthen
adaptation
to
life
circumstances,
and
lead
to
individual
and
interpersonal
improvement
and
increased
satisfaction
with
marriage
and
family
life
in
these
families.
Life
skills
training
could
lead
to
positive
effects
on
mental
and
physical
status
and
marital
satisfaction
in
veterans’
wives.
The
important
implication
of
the
present
study
was
that
life
skills
should
be
educated
continuously
for
veterans
and
their
families
because
the
participants
had
recurrent
symptoms
and
problems
in
the
follow-up.
Unfortunately,
veterans’
families
have
been
recently
abandoned
unaided
and
only
Counseling
Center
of
Martyr
Foundation
is
delivering
individual
and
voluntary
services
to
these
families.
In
contrast,
most
of
the
necessary
training
for
such
families
should
be
conducted
in
a
group,
continuously,
and
depending
on
the
type
of
disability.
This
issue
is
more
urgent
for
the
families
with
veterans
with
more
severe
disability
and
neurological
problems.
Further
studies
are
recommended
to
study
the
effect
of
psychological
interventions
on
veterans’
wives
and
other
family
members
depending
on
the
type
of
their
injuries.
Veterans
suffer
from
different
types
of
handicaps
and
therefore
their
families,
including
wives,
are
variously
affected.
For
example,
the
effects
on
the
family
of
a
veteran
with
PTSD
may
be
widely
different
from
those
on
the
family
of
a
veteran
with
a
handicap
from
shooting.
However,
we
decided
to
enroll
veterans
with
different
types
of
handicaps
to
have
an
adequate
sample
size.
Consequently,
the
findings
should
be
cautiously
interpreted
and
generalized.
Acknowledgements:
The
author
sincerely
thanks
all
people
who
cooperated
with
this
study.
1.
WHO.
Programme
on
mental
health,
Life
skills
education
in
schools.
Division
of
mental
health
and
prevention
of
substance
abuse.
1997;Geneva:1.
2.
Nikfarjam
M,
SolatiDehkordi
K,
Aghaei
A,
Rahimian
G.
Efficacy
of
hypnotherapy
in
conjunction
with
pharmacotherapy
and
pharmacotherapy
alone
on
the
quality
of
life
in
patients
with
irritable
bowel
syndrome.
Govaresh.
2013;18(3):149-56.
3.
Haghayegh
SA,
Neshatdoost
H,
Drossman
DA,
Asgari
K,
Soulati
SK,
Adibi
P.
Psychometric
Characteristics
of
the
Persian
Version
of
the
Irritable
Bowel
Syndrome
Quality
of
Life
Questionnaire
(P-IBS-QOL).
Pakistan
Journal
of
Medical
Sciences.
2012;8(2):312-7.
4.
Solati
K.
Effectiveness
of
cognitive-behavior
group
therapy,
psycho-education
family,
and
drug
therapy
in
reducing
and
preventing
recurrence
of
symptoms
in
patients
with
major
depressive
disorder.
Journal
of
Chemical
and
Pharmaceutical
Sciences.
2016;2(40.84):3.55.
5.
Asadi
Noghabi
AA,
Zandi
M,
Mehran
A,
Alavian
SM,
Dehkordi
AH.
The
Effect
of
Education
on
Quality
of
Life
in
Patients
under
Interferon
Therapy.
Hepatitis
Monthly.
2010:10(3):218-22.
PubMed
PMID:
PMC3269087.
6.
Solati
K,
Lo’Bat
Ja’Farzadeh
AH.
The
effect
of
stress
management
based
on
group
cognitive-behavioural
therapy
on
marital
satisfaction
in
infertile
women.
Journal
of
clinical
and
diagnostic
research:
2016;10(7):VC01.
7.
Solati
K.
The
Efficacy
of
Mindfulness-Based
Cognitive
Therapy
on
Resilience
among
the
Wives
of
Patients
with
Schizophrenia.
Journal
of
clinical
and
diagnostic
research:
2017;11(4):VC01.
8.
Dehkordi
AH,
Solati
K.
The
effects
of
cognitive
behavioral
therapy
and
drug
therapy
on
quality
of
life
and
symptoms
of
patients
with
irritable
bowel
syndrome.
Journal
of
advanced
pharmaceutical
technology
&
research.
2017;8(2):67.
9.
Solati
Dehkordy
K,
Adibi
P,
Sobhi
Gharamaleky
N.
Effects
of
relaxation
and
citalopram
on
severity
and
frequency
of
the
symptoms
of
irritable
bowel
syndrome
with
diarrhea
predominance.
Pakistan
Journal
of
Medical
Sciences.
2010;26(1):88-91.
Pakistan
Journal
of
Medical
Sciences.
2010;26(1):88-91.
10.
Elbogen
EB,
Fuller
S,
Johnson
SC,
Brooks
S,
Kinneer
P,
Calhoun
PS,
et
al.
Improving
risk
assessment
of
violence
among
military
veterans:
an
evidence-based
approach
for
clinical
decision-making.
Clinical
psychology
review.
2010
Aug;30(6):595-607.
PubMed
PMID:
20627387.
Pubmed
Central
PMCID:
2925261.
11.
Galovski
T,
Lyons
JA.
Psychological
sequelae
of
combat
violence:
A
review
of
the
impact
of
PTSD
on
the
veteran’s
family
and
possible
interventions.
Aggression
and
Violent
Behaviour.
2004;9(5):477–501.
12.
King
DW,
Taft
C,
King
LA,
Hammond
C,
Stone
ER.
Directionality
of
the
Association
Between
Social
Support
and
Posttraumatic
Stress
Disorder:
A
Longitudinal
Investigation.
Journal
of
applied
social
psychology.
2006;36(12):2980-92.
13.
Nichols
LO,
Martindale-Adams
J,
Graney
MJ,
Zuber
J,
Burns
R.
Easing
reintegration:
telephone
support
groups
for
spouses
of
returning
Iraq
and
Afghanistan
service
members.
Health
communication.
2013;28(8):767-77.
PubMed
PMID:
24134192.
14.
Renshaw
KD,
Rodrigues
CS,
Jones
DH.
Psychological
symptoms
and
marital
satisfaction
in
spouses
of
Operation
Iraqi
Freedom
veterans:
relationships
with
spouses’
perceptions
of
veterans’
experiences
and
symptoms.
Journal
of
family
psychology:
2008
Aug;22(4):586-94.
PubMed
PMID:
18729672.
15.
Ahmadi
K,
Ranjebar-Shayan
H,
Raiisi
F.
Sexual
dysfunction
and
marital
satisfaction
among
the
chemically
injured
veterans.
Indian
journal
of
urology.
2007
Oct;23(4):377-82.
PubMed
PMID:
19718292.
Pubmed
Central
PMCID:
2721568.
16.
Ahmadi
K,
Fathi-Ashtiani
A,
Zareir
A,
Arabnia
A,
Amiri
M.
Sexual
dysfunctions
and
marital
adjustment
in
veterans
with
PTSD.
Archives
of
Medical
Science.
2006;2(4):280-5.
17.
Lyubomirsky
S,
King
L,
Diener
E.
The
benefits
of
frequent
positive
affect:
does
happiness
lead
to
success?
Psychological
bulletin.
2005
Nov;131(6):803-55.
PubMed
PMID:
16351326.
18.
Lyubomirsky
S,
Tkach
C,
DiMatteo
MR.
What
are
the
differences
between
happiness
and
self-esteem.
Social
Indicators
Research.
2006;78(3):363-404.
19.
Kaplan
M,
Maddux
JE.
Goals
and
marital
satisfaction:
Perceived
support
for
personal
goals
and
collective
efficacy
for
collective
goals.
Journal
of
Social
and
Clinical
Psychology.
2002;21(2):157-64.
20.
Kim
GS,
Kim
B,
Moon
SS,
Park
CG,
Cho
YH.
Correlates
of
depressive
symptoms
in
married
immigrant
women
in
Korea.
Journal
of
transcultural
nursing
:
official
journal
of
the
Transcultural
Nursing
Society
/
Transcultural
Nursing
Society.
2013
Apr;24(2):153-61.
PubMed
PMID:
23341405.
21.
Miller
RB,
Mason
TM,
Canlas
JM,
Wang
D,
Nelson
DA,
Hart
CH.
Marital
satisfaction
and
depressive
symptoms
in
China.
Journal
of
family
psychology
:
JFP
:
journal
of
the
Division
of
Family
Psychology
of
the
American
Psychological
Association.
2013
Aug;27(4):677-82.
PubMed
PMID:
23834363.
22.
Klaric
M,
Franciskovic
T,
Stevanovic
A,
Petrov
B,
Jonovska
S,
Nemcic
Moro
I.
Marital
quality
and
relationship
satisfaction
in
war
veterans
and
their
wives
in
Bosnia
and
Herzegovina.
European
journal
of
psychotraumatology.
2011;2.
PubMed
PMID:
22893809.
Pubmed
Central
PMCID:
3402112.
23.
Afkar
AH,
Mahbobubi
M,
Neyakan
Shahri
M,
Mohammadi
M,
Jalilian
F,
Moradi
F.
Investigation
of
the
relationship
between
illogical
thoughts
and
dependence
on
others
and
marriage
compatibility
in
the
Iranian
Veterans
exposed
to
chemicals
in
Iran-Iraq
War.
Global
journal
of
health
science.
2014
Sep;6(5):38-45.
PubMed
PMID:
25168982.
24.
Sepulveda
AR,
Lopez
C,
Macdonald
P,
Treasure
J.
Feasibility
and
acceptability
of
DVD
and
telephone
coaching-based
skills
training
for
carers
of
people
with
an
eating
disorder.
The
International
journal
of
eating
disorders.
2008
May;41(4):318-25.
PubMed
PMID:
18176950.
25.
Magnani
R,
Macintyre
K,
Karim
AM,
Brown
L,
Hutchinson
P,
Kaufman
C,
et
al.
The
impact
of
life
skills
education
on
adolescent
sexual
risk
behaviors
in
KwaZulu-Natal,
South
Africa.
The
Journal
of
adolescent
health
:
official
publication
of
the
Society
for
Adolescent
Medicine.
2005
Apr;36(4):289-304.
PubMed
PMID:
15780784.
26.
Botvin
G,
Griffin
K.
Life
skills
training:
Empirical
findings
and
future
directions.
Journal
of
Primary
Prevention.
2004;25(2):211-32.
27.
Gorman
DM.
Does
measurement
dependence
explain
the
effects
of
the
Life
Skills
Training
program
on
smoking
outcomes?
Preventive
medicine.
2005
Apr;40(4):479-87.
PubMed
PMID:
15530601.
28.
Codony
M,
Alonso
J,
Almansa
J,
Bernert
S,
de
Girolamo
G,
de
Graaf
R,
et
al.
Perceived
need
for
mental
health
care
and
service
use
among
adults
in
Western
Europe:
results
of
the
ESEMeD
project.
Psychiatric
services.
2009
Aug;60(8):1051-8.
PubMed
PMID:
19648192.
29.
Pick
S,
Givaudan
M,
Poortinga
YH.
Sexuality
and
life
skills
education.
A
multistrategy
intervention
in
Mexico.
The
American
psychologist.
2003
Mar;58(3):230-4.
PubMed
PMID:
12772430.
30.
Taft
CT,
Street
AE,
Marshall
AD,
Dowdall
DJ,
Riggs
DS.
Posttraumatic
stress
disorder,
anger,
and
partner
abuse
among
Vietnam
combat
veterans.
Journal
of
family
psychology
:
JFP
:
journal
of
the
Division
of
Family
Psychology
of
the
American
Psychological
Association.
2007
Jun;21(2):270-7.
PubMed
PMID:
17605549.
31.
Weine
S,
Ukshini
S,
Griffith
J,
Agani
F,
Pulleyblank-Coffey
E,
Ulaj
J,
et
al.
A
family
approach
to
severe
mental
illness
in
post-war
Kosovo.
Psychiatry.
2005
Spring;68(1):17-27.
PubMed
PMID:
15899707.
32.
Siamian
H,
Naeimi
O,
Shahrabi
A,
Hassanzadeh
R,
Abazari
M,
Khademloo
M,
et
al.
The
Status
of
Happiness
and
its
Association
with
Demographic
Variables
among
the
Paramedical
Students.
J
Mazandaran
Univ
Med
Sci.
2012;21
(86):159-66.
33.
Argyle
M,
Martin
M,
Crossland
J.
Happiness
as
a
function
of
personality
and
social
encounters.
In:
Forgas
JP,
Innes
JM
(Eds).
Recent
advances
in
social
psychology:
An
international
perspective.
Netherlands:
Elsevier
Science
Publishers.
1989:189-203.
34.
Alipoor
A,
Noorbala
A.
A
Preliminary
Evaluation
of
the
Validity
and
Reliability
of
the
Oxford
Happiness
Questionnaire
in
Students
in
the
Universities
of
Tehran.
Iranian
Journal
of
Psychiatry
and
Clinical
Psychology.
1999;5(1&2):55-66.
35.
Goldberg
DP,
Hillier
VF.
A
scaled
version
of
the
General
Health
Questionnaire.
Psychological
medicine.
1979
Feb;9(1):139-45.
PubMed
PMID:
424481.
36.
Jenkins
R,
Elliott
P.
Stressors,
burnout
and
social
support:
nurses
in
acute
mental
health
settings.
Journal
of
Advanced
Nursing.
2004;48(6):622-31.
37.
Williams
P,
Goldberg
DP,
Mari
J.
The
validity
of
the
GHQ-28.
Social
Psychiatry.
1987;21:15-8.
38.
Ebrahimi
A,
Moulavi
H,
Mousavi
S,
Bornamanesh
A,
Yaghoubi
M.
Psychometric
properties
and
factor
structure
of
General
Health
Questionnaire
28
(GHQ-28)
in
Iranian
psychiatric
patients.
Journal
of
Research
in
Behavioural
Sciences.
2007;5(1):5-12.
39.
Fowers
B,
Olson
D.
ENRICH
Marital
Satisfaction
Scale:
A
brief
research
and
clinical
tool.
Journal
of
family
psychology
:
JFP
:
journal
of
the
Division
of
Family
Psychology
of
the
American
Psychological
Association.
1993;7(2):176-85.
40.
Kees
M,
Rosenblum
K.
Evaluation
of
a
psychological
health
and
resilience
intervention
for
military
spouses:
A
pilot
study.
Psychological
services.
2015;12(3):222.
41.
Elliott
TR,
Berry
JW,
Grant
JS.
Problem-solving
training
for
family
caregivers
of
women
with
disabilities:
a
randomized
clinical
trial.
Behaviour
research
and
therapy.
2009
Jul;47(7):548-58.
PubMed
PMID:
19361781.
Pubmed
Central
PMCID:
2737710.
42.
Layne
CM,
Saltzman
WR,
Poppleton
L,
Burlingame
GM,
Pasalic
A,
Durakovic
E,
et
al.
Effectiveness
of
a
school-based
group
psychotherapy
program
for
war-exposed
adolescents:
a
randomized
controlled
trial.
Journal
of
the
American
Academy
of
Child
and
Adolescent
Psychiatry.
2008
Sep;47(9):1048-62.
PubMed
PMID:
18664995.
43.
Hojjat
Sk,
Hatami
SE,
Rezaei
M,
Khalili
MN,
Talebi
MR.
The
efficacy
of
training
of
stress-coping
strategies
on
marital
satisfaction
of
spouses
of
veterans
with
post-traumatic
stress
disorder.
Electronic
Physician.
2016;8(4):2232-7.
PubMed
PMID:
PMC4886563.
44.
Ray
SL,
Vanstone
M.
The
impact
of
PTSD
on
veterans’
family
relationships:
an
interpretative
phenomenological
inquiry.
International
journal
of
nursing
studies.
2009
Jun;46(6):838-47.
PubMed
PMID:
19201406.
45.
Monson
CM,
Taft
CT,
Fredman
SJ.
Military-related
PTSD
and
Intimate
Relationships:
From
Description
to
Theory-Driven
Research
and
Intervention
Development.
Clinical
psychology
review.
2009
09/10;29(8):707-14.
PubMed
PMID:
PMC2783889.
46.
Sullivan
CP,
Elbogen
EB.
PTSD
Symptoms
and
Family
vs.
Stranger
Violence
in
Iraq
and
Afghanistan
Veterans.
Law
and
human
behavior.
2014
05/06;38(1):1-9.
PubMed
PMID:
PMC4394858.
47.
Reisman
M.
PTSD
Treatment
for
Veterans:
What’s
Working,
What’s
New,
and
What’s
Next.
Pharmacy
and
Therapeutics.
2016;41(10):623-34.
PubMed
PMID:
PMC5047000.
|

