|
|
 |
| ............................................................. |
|
|
| ........................................................ |
| From
the Editor |

|
Editorial
A. Abyad (Chief Editor)
DOI:10.5742/MEWFM.2019.93610
|
........................................................
|
|
Editorial
Dr.
Abdulrazak Abyad
DOI: 10.5742/MEWFM.2019.93623
Original Contribution
Self-monitoring
of Blood Glucose Among Type-2 Diabetic Patients:
An Analytical Cross-Sectional Study
[pdf]
Ahmed S. Alzahrani, Rishi K. Bharti, Hassan
M. Al-musa, Shweta Chaudhary
DOI: 10.5742/MEWFM.2019.93624
White
coat hypertension may actually be an acute phase
reactant in the body
[pdf]
Mehmet Rami Helvaci, Orhan Ayyildiz, Orhan Ekrem
Muftuoglu, Mehmet Gundogdu, Abdulrazak Abyad,
Lesley Pocock
DOI: 10.5742/MEWFM.2019.93625
Case Report
An
Unusual Persistent Mullerian Duct Syndrome in
a child in Abha city: A Case Report
[pdf]
Youssef Ali Mohamad Alqahtani, Abdulrazak Tanim
Abdulrazak, Hassa Gilban, Rasha Mirdad, Ashwaq
Y. Asiri, Rishi Kumar Bharti, Shweta Chaudhary
DOI: 10.5742/MEWFM.2019.93628
Population and Community
Studies
Prevalence
of abdominal obesity and its associated comorbid
condition in adult Yemeni people of Sana’a
City
[pdf]
Mohammed Ahmed Bamashmos
DOI: 10.5742/MEWFM.2019.93626
Smoking
may even cause irritable bowel syndrome
[pdf]
Mehmet Rami Helvaci, Guner Dede, Yasin Yildirim,
Semih Salaz, Abdulrazak Abyad, Lesley Pocock
DOI: 10.5742/MEWFM.2019.93629
Systematic
literature review on early onset dementia
[pdf]
Wendy Eskine
DOI: 10.5742/MEWFM.2019.93627
|
|
Chief
Editor -
Abdulrazak
Abyad
MD, MPH, MBA, AGSF, AFCHSE
.........................................................
Editorial
Office -
Abyad Medical Center & Middle East Longevity
Institute
Azmi Street, Abdo Center,
PO BOX 618
Tripoli, Lebanon
Phone: (961) 6-443684
Fax: (961) 6-443685
Email:
aabyad@cyberia.net.lb
.........................................................
Publisher
-
Lesley
Pocock
medi+WORLD International
AUSTRALIA
Email:
lesleypocock@mediworld.com.au
.........................................................
Editorial
Enquiries -
abyad@cyberia.net.lb
.........................................................
Advertising
Enquiries -
lesleypocock@mediworld.com.au
.........................................................
While all
efforts have been made to ensure the accuracy
of the information in this journal, opinions
expressed are those of the authors and do not
necessarily reflect the views of The Publishers,
Editor or the Editorial Board. The publishers,
Editor and Editorial Board cannot be held responsible
for errors or any consequences arising from
the use of information contained in this journal;
or the views and opinions expressed. Publication
of any advertisements does not constitute any
endorsement by the Publishers and Editors of
the product advertised.
The contents
of this journal are copyright. Apart from any
fair dealing for purposes of private study,
research, criticism or review, as permitted
under the Australian Copyright Act, no part
of this program may be reproduced without the
permission of the publisher.
|
|
|
| March 2019 - Volume
17, Issue 3 |
|
|
Early Onset Dementia: A Systematic
Review of the Literature to Inform Qualitative
Experiences
Wendy Erskine
Correspondence:
Wendy
Erskine BA, LLB, A.B.P.I., M.Litt PhD.
St Andrews,
Fife,
Scotland
Email: wendy.erskine2014@gmail.com
Received: January 2019; Accepted: February
2019; Published: March 1, 2019
Citation: Wendy Erskine. Early Onset Dementia:
A Systematic Review of the Literature to Inform
Qualitative Experiences. World Family Medicine.
2019; 17(3): 34-58. DOI: 10.5742/MEWFM.2019.93627
|
Abstract
There is increasing recognition that EOD
(Early Onset Dementia) represents an important
social problem affecting economic and
social impacts (Campbell et al., 2008;
Johannessen et al., 2018). Recent research
calls for greater efforts to be made in
consulting with the PwD (people with dementia)
directly (Allen 2001; Bamford & Bruce
2000). The condition is understood to
occur between the ages of 45-65 (Mercy,
2008). This makes EOD a sub-group of dementia
with numerous differences when compared
to later onset dementia. These include
the likelihood of still being in work
and having a family to raise. Being responsible
for an income and for dependent others
is particularly difficult for those affected.
Additionally, the social and psychological
context for younger people is different
(Beattie, 2004). PwEOD (people with Early
Onset Dementia) are more likely to be
physically fitter than those with later
onset dementia which may impact on their
physical care needs. The existing expectation
within health and social care agencies
for PwEOD is in keeping within an older
person’s framework of care which
may well be inappropriate. This may have
occurred in the past due to biomedical
assumptions regarding the condition (Kitwood,
1997; van Vliet et al., 2017). This also
suggests that little attention has been
paid to subjective experiences (van Vliet,
2017). The need to elicit the views and
subjective experiences of PwEOD is therefore
gaining increasing recognition within
health and social care research (van Vliet,
2010). Literature has been modestly growing
in the subject area to demonstrate how
PwEOD have expressed their views and experience
of dementia successfully (Page and Keady,
2010; Ohman et al., 2001). However, most
of the extant literatureis based on family
carers (Cabote, 2015; Kobiske and Bekhet,
2018). Whilst carers’ views are important
they should not be used as a substitute
for the views of younger people with dementia
(Goldsmith 1996, Whitlatch 2001). Given
the limited research available, both the
views of PwEOD and their family carers
are incorporated into the systematic literature
review.
Key words:
Early onset dementia (EOD), qualitative,
people with early onset dementia (PwEOD),
family kin, meta-ethnography, stigma,
liminality and chronicity, biographical
disruption, losses, coping
|
Personal accounts describing EOD have potential
to inform clinical and care provision as well
as informing other dementia subsets. Examining
first person accounts makes this a valuable
exercise. This may be assumed as PwEOD (People
with Early Onset Dementia) possess more faculties
with which to tell about lived experience from
first person accounts.
Study
aim:
This
systematic
review
paper
sought
to
address
the
following
question:
‘How
do
PwEOD
as
a
diagnosed
sub
group
of
other
dementias
and
their
immediate
family
experience
living
with
EOD?’
Study
inclusion:
Studies
were
included
and
excluded
according
to
the
following
criteria:
a
diagnosis
of
EOD
between
the
ages
of
45-65
[1];
research
dated
between
1998-2018;[2]
in
English
language;
qualitative
and
peer
reviewed
papers.
The
key
aim
of
study
inclusion
was
to
capture
the
experience
of
living
with
EOD
through
the
available
literature
in
the
field.
Personal
experiences
were
sought
in
the
literature
on
PwEOD
and
their
immediate
family
living
with
the
experience
post-diagnosis.
The
scoping
review
uncovered
the
relative
lack
of
studies
to
date
on
the
experiences
of
PwEOD,
therefore
studies
were
inclusive
of
spouses,
partners,
children
and
adult
dependents
as
people
living
with
the
PwEOD.
Searches
were
kept
broad
and
unconstrained
by
further
filters
in
order
to
capture
a
fuller
picture
of
the
issues
and
experiences
connected
to
EOD.
Study
exclusion:
Studies
focusing
solely
on
people
presenting
with
dementia
younger
than
45;
studies
with
a
predominant
interest
in;
dementia
caused
by
HIV,
traumatic
brain
injury,
Down’s
syndrome,
congenital
birth
conditions
likely
to
include
dementia,
Huntington’s
chorea
and
alcohol-related
dementia
were
excluded.
Systematic
literature
reviews
were
excluded.
Scoping:
A
scoping
exercise
of
the
literature
took
place
prior
to
the
systematic
literature
review
which
identified
EOD
as
a
sub-group
of
dementia
under-represented
in
the
literature.
Google
Scholar
and
Abertay’s
Library
Search
including
serendipitous
searches
using
prior
knowledge
of
the
research
field
extended
the
search
in
preparation
for
the
systematic
review.
Search
strategy:
The
author
then
searched
databases
which
were
selected
for
their
social
and
clinical
perspectives
through
EBSCOhost;
Web
of
Science
and
Cinahl
plus
with
text,
Psychology
and
Behavioural
Sciences
Collection,
Scopus
and
Sage.
The
search
terms
were:
dement*,
early
onset
dementia,
young
onset
dementia,
presenile-Alzheimer*
and
working
age
dementia.
These
were
searched
as
single
terms
using
Boolean
phrasing;
‘OR’
then
once
the
searches
were
captured,
refined
with;
‘AND’
then
stored
for
scrutiny
at
the
next
stage.
Selection
of
papers:
The
search
located
five-hundred-and-fifty-two
(522)
papers.
Duplicates
were
removed
(n=22).
The
remaining
studies’
(n=500)
abstracts
and
titles
were
screened.
Twenty-two
studies
(n=22)
were
retained
and
full
texts
read.
This
left
sixteen
studies
(n=16)
to
be
included.
The
reference
lists
of
the
twenty-two
studies
were
also
examined.
Although
two
were
added
from
references,
they
were
finally
excluded
for
failing
to
meet
the
criteria.
With
reference
to
the
final
six
studies
excluded,
these
are
listed
in
the
appendices
(Appendix
1).
Approach
to
systematic
and
meta-analysis
synthesis
of
studies
The
review
was
guided
by
the
systematic
approach
preferred
by
PRISMA
(Reporting
Systematic
Reviews
and
Meta-Analysis
Studies
(Liberati,
2009).
Figure
1
illustrates
the
process
of
papers
being
excluded
or
included
for
the
systematic
review
based
upon
the
study
question.
This
process
sets
a
standard
for
the
assessment
and
critique
of
health
focussed
studies
and
interventions
assisting
the
processes
for
summarising
evidence
accurately
and
reliably.
However,
it
is
the
case
that
the
methods
of
meta-analysis
are
not
transferable
to
qualitative
health
research
for
a
number
of
pragmatic
and
epistemological
reasons;
for
example,
computer
literature
searches,
statistical
data
and
priorities
in
quantitative
research
may
fail
to
capture
forms
of
qualitative
research
which
lack
the
appeal
of
more
clinical
protocols
and
interventions
(Britten
et
al.,
2002).
As
such,
criteria
for
judging
the
quality
of
published
research
whilst
contested
in
the
past
have
since
found
established
qualitative
protocols
for
comparing
studies
(Britten
et
al.,
2002).
The
potential
audiences
for
viewing
research
through
this
lens
include
practitioners
across
a
broad
health
practice
background
as
well
as
policy-makers
and
qualitative
researchers
(Britten
et
al.,
2002).
Therefore,
there
exists
several
well
recognised
methods
by
which
to
conduct
a
systematic
review
of
qualitative
literature
(Greenwood
&
Smith,
2016).
The
role
of
meta-ethnography
in
qualitative
research
The
impetus
for
developing
methods
of
qualitative
synthesis
has
arisen
from
a
need
to
complement
quantitative
research.
This
looked
to
gain
a
more
complete
understanding
of
phenomena,
especially
in
terms
of
organisational
processes
and
provision
of
services
(Greenhalgh,
1998).
Therefore
a
need
existed
to
bring
together
isolated
studies
for
comparison
(Sandelowski
et
al.,
1997).
Meta-ethnography
provides
a
way
to
compare
qualitative
studies
accommodating
induction
and
interpretation
(Greenwood
&
Smith,
2016).
It
also
can
synthesise
conceptual
innovations
such
as
metaphorical
and
emotionally
relevant
phenomena
(Strike
and
Posner,
1983).
It
has
origins
in
the
interpretive
paradigm
and
as
such,
it
possesses
an
alternative
to
traditional
aggregative
methods
of
synthesis
which
retain
qualities
or
concepts
of
the
qualitative
method
of
study
it
aims
to
synthesise.
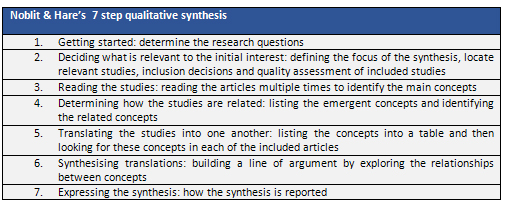
The
benefit
of
applying
meta-ethnography
to
the
synthesis
of
qualitative
research
and
suitability
for
this
study
was
informed
by
Noblit
and
Hare’s
(1988)
seven-step
process
(Table
1).
Narrative
literature
reviews
capture
concepts
and
information
in
a
more
eclectic
fashion
but
have
in
the
past
been
criticised
for
being
singular
descriptive
accounts
based
upon
the
implicit
bias
of
the
researcher
(Fink,
1998).
They
have
also
been
condemned
for
lacking
critical
assessment.
Adopting
a
more
systematic
approach
to
the
literature
was
therefore
useful
in
order
to
approach
a
more
comprehensive
contemporary
review
of
the
field.
This
approach
was
particularly
helpful
in
investigating
EOD
as
a
lesser
known
sub-group
of
dementia.
Meta-ethnography
has
proven
a
sound
technique
for
synthesising
qualitative
research
in
health
studies
(Paterson
et
al.,
1998).
It
has
been
successfully
employed
in
publications
to
date
including:
lay
meanings
of
medicines
(Britten
et
al.,
(2002);
lay
experiences
of
diabetes
and
diabetes
care
(Campbell
et
al;
2003);
what
values
people
seek
when
they
provide
unpaid
care
for
an
older
person
(Al-Janabi
et
al.,
2008)
and
locating
how
coping
experiences
appear
in
chronic
fatigue
syndrome
sufferers
(Larun
and
Malterud,
2007).
[1]
This
definition
is in
keeping
with
Mercy
(2008),
excluding
two
other
studies
limiting
EOD
to 45-60.
All
others
searched
for
the
systematic
review
including
the
scoping
review
referred
to 45-65
as the
most
commonly
used
criteria
for
EOD.
[2]
Searches
between
1998-2018
captured
the
advent
and
widespread
prescription
of anti-cholinesterase
inhibitor
treatment
and
linked
with
a key
driver
as laid
out
in the
Scottish
Government’s
2009
report
making
dementia
a healthcare
priority
for
development.
Table
1:
Click
here
for
Figure
1:
PRISMA
flowchart
Participant
and
study
design
The
inclusion
criteria
sought
studies
spanning
1998-2018.
However,
the
studies
ranged
from
2009
to
2018.
The
mean
date
was
2015.
All
studies
were
performed
in
Western
countries
(Norway-6;
America-1;
England-;
6;
The
Netherlands-1;
Ireland-1
&
Australia-1).
Where
English
was
not
the
dominant
language
it
was
widely
taught
and
well
spoken
(Norway
and
The
Netherlands).
The
participants
were
predominantly
drawn
from
health
environments
or
services
structured
to
assist
PwD
or
PwEOD
such
as
statutory
or
voluntary
bodies.
There
were
a
total
of
229
participants
after
making
amendments
for
those
participants
drawn
from
the
same
sample
groups
where
multiple
study
authors
were
included.
Johannessen
et
al.,
(2014)
and
Johannessen
and
Moller
(2011)
used
the
same
participants.
Johannessen
et
al.,
(2016)
and
Johannessen
et
al.,
(2017)
also
shared
participants
databases
throughout
the
studies.
Data
were
collected
through
face
to
face
interview
mostly
using
a
semi-structured
format.
These
were
situated
within
the
statistics
of
the
studies
quoted
above;
(PwEOD
(4);
their
family
members
(2);
both
spouses
(2)
and
dependents
(8)
whether
still
regarded
as
children
living
at
home
or
adult
children
living
independently
elsewhere).
These
studies
drew
together
the
theoretical
approaches
to
the
data
founded
in:
grounded
theory
(5);
autobiographical
life
story
narrative
(3);
phenomenological
hermeneutic
analysis
(2);
Thematic
Analysis
(TA)
(2);
qualitative
semi
structured
interview
(1);
conceptual
model
(1);
action
research
study
(1)
Interpretative
phenomenological
analysis
(IPA)
(1).
Ethnicity
was
referred
to
infrequently
(n=1)
and
where
ethnic
origins
were
detailed,
the
sample
groups
were
white/Western.
Allen
et
al.,
(2009)
was
the
only
study
to
include
25%
Asian
participants
within
an
English
sample.
Other
studies
made
no
attempt
to
refer
to
ethnicity
and
so
a
presumption
is
made
that
natives
of
the
country
of
origin
satisfied
the
sample
cohorts.
This
is
excepting
Sikes
and
Hall
(2017)
which
reported
that
the
sample
participant
group
was
‘mainly
white,
British,
middle-class,
participants’.
Type
of
dementia
was
not
a
focus
except
for
Johannessen
et
al.,
(2017)
which
focused
on
people
with
fronto-temporal
lobe
dementia.
Other
data
reported
were
related
to
whether
participants
(both
PwEOD
and
family)
were
working,
living
at
home,
in
studies,
in
a
care
home,
retired
or
medically
signed
off
work
and
living
on
retirement
funds
or
state
benefits.
The
source
for
participants
overwhelmingly
arose
from
clinical
or
health
focused
environments.
This
particular
feature
was
examined
in
the
discussion
of
the
studies.
Having
noted
the
brief
characteristics
of
the
studies
above,
the
following
tables
and
sub-sections
developed
overall
themes
along
with
the
development
of
the
line
of
argument.
Click
here
for
Table
2:
Participant
and
study
design
Drawing
a
line
of
argument
from
the
seven
step
process
Noblet
and
Hare
(1988)
refer
to
a
meta-ethnographic
line
of
argument
which
emerges
to
articulate
a
larger
phenomenon
drawn
from
the
data.
This
was
achieved
by
following
the
steps.
After
selecting
an
aim
and
study
question
(steps
one
and
two),
the
studies
were
read
to
fulfil
step
three.
This
was
followed
by
populating
the
tables
with
typical
broad
characteristics
(Table
2).
Investigation
of
experiences
were
then
described
(Table
3).
Following
this,
steps
four,
five
and
six
produced
more
concepts
(Table
4)
and
themes
(Table
5)
were
populated
taking
care
to
ensure
the
data
remained
true
to
the
original
studies.
Step
seven
provided
for
a
discussion
through
the
line
of
argument
of
what
fresh
data
was
discovered.
Click
here
for
Table
3:
Investigation
of
experiences
Overall
themes
By
the
time
Table
five
was
completed
at
stages
five
and
six
in
accordance
with
Noblit
and
Hare’s
seven
step
process,
new
data
emerged
to
realise
conceptual
themes
crystallised
into
themes
which
formed
the
expression
of
the
new
information.
The
expression
of
the
synthesis
followed
the
tables
discussed
theme
by
theme.
Click
here
for
Table
4:
Conceptual
themes
Conceptual
themes
and
Schultz’s
first
and
second
order
constructs
The
table
below
concluded
the
development
of
the
line
of
argument.
Noblit
and
Hare
adopted
Schutz’s
notion
of
first
and
second
order
constructs
assisting
the
progression
of
themes.
Schutz
utilised
the
term
first-order
construct
in
referring
to
the
everyday
constructs
and
understandings
of
ordinary
lay
people.
The
second-order
construct
referred
to
those
constructs
familiar
to
social
science
researchers.
The
table
below
(Table
5)
reveals
how
the
themes
took
their
place
within
the
constructs
drawn
in
accordance
with
Schutz’s
terms.
The
final
themes
that
arose
were:
i)
biographical
disruption
ii)
diagnosis,
iii)
losing
life,
friends
and
competences,
iv)
liminality
and
chronicity,
v)
stigma,
and
vi)
coping
with
cautious
optimism.
The
table
below
finalised
the
creation
of
new
concepts
which
are
followed
by
discussion
of
the
themes.
Click
here
for
Table
5:
Second
and
third
order
interpretations
| | |
