|
|
 |
Medicine and Society
........................................................
Case Report
........................................................
Continuing Education
|
Chief
Editor -
Abdulrazak
Abyad
MD, MPH, MBA, AGSF, AFCHSE
.........................................................
Editorial
Office -
Abyad Medical Center & Middle East Longevity
Institute
Azmi Street, Abdo Center,
PO BOX 618
Tripoli, Lebanon
Phone: (961) 6-443684
Fax: (961) 6-443685
Email:
aabyad@cyberia.net.lb
.........................................................
Publisher
-
Lesley
Pocock
medi+WORLD International
11 Colston Avenue,
Sherbrooke 3789
AUSTRALIA
Phone: +61 (3) 9005 9847
Fax: +61 (3) 9012 5857
Email:
lesleypocock@mediworld.com.au
.........................................................
Editorial
Enquiries -
abyad@cyberia.net.lb
.........................................................
Advertising
Enquiries -
lesleypocock@mediworld.com.au
.........................................................
While all
efforts have been made to ensure the accuracy
of the information in this journal, opinions
expressed are those of the authors and do not
necessarily reflect the views of The Publishers,
Editor or the Editorial Board. The publishers,
Editor and Editorial Board cannot be held responsible
for errors or any consequences arising from
the use of information contained in this journal;
or the views and opinions expressed. Publication
of any advertisements does not constitute any
endorsement by the Publishers and Editors of
the product advertised.
The contents
of this journal are copyright. Apart from any
fair dealing for purposes of private study,
research, criticism or review, as permitted
under the Australian Copyright Act, no part
of this program may be reproduced without the
permission of the publisher.
|
|
|
| January 2015 -
Volume 13 Issue 1 |
|
Increasing
incidences of STIs in Pakistani youth; Role of
Family Physicians in prevention, treatment and
control of STIs
Manzoor Butt
Correspondence:
Dr Manzoor Ahmed Butt
Rawalpindi, Pakistan
Email:
drmanzoor@ymail.com
|
Background
Sexually
transmitted infections (STIs) constitute
a major cause of acute illness, infertility,
long-term disability and death, with severe
medical and psychological consequences
for millions of men, women and infants.
In Pakistan, the STIs control programme
focuses on infections such as syphilis,
chancroid, gonorrhoea, chlamydial infection,
trichomoniasis, and their associated syndromes.
Viral infections like herpes simplex viruses
(HSV) and human papilloma viruses (HPV)
are also included in these programmes
as these are usually transmitted sexually.
|
This article describes STIs in Pakistan. STIs
are some of the most common causes of illness
worldwide. STIs accounted for 87% of all cases,
reported among the top 10 most frequently reported
diseases in 1995. STIs are more common in developing
countries than industrial countries. In many
developing countries, STIs rank among the top
five diseases.[1] Incidence of STIs is rising
despite improved methods of diagnosis and treatment.
[2] There are 333 million new cases of STIs
(excluding human immunodeficiency virus (HIV)
and AIDS) per year globally. In 1995 in South
East Asia alone an estimated 150 million new
cases occurred [3].
|
EPIDEMIOLOGY
AND
CURRENT
SITUATION
IN
PAKISTAN |
It is usually said that
the incidence of STIs
in Pakistan is very low
among the general population.
The author does not agree
with this statement. In
fact, there is no exact
data available about STIs
in Pakistan as these are
not notified to any authority.
There is no STIs reporting
system in Pakistan and
therefore information
about STIs prevalence
is limited.[4] Gonorrhoea
and syphilis are more
common STIs in Pakistan
[5], but gonorrhoea is
the most pressing and
emerging infection in
the youth and very young
boys of our communities.
Pakistan is facing a
growing problem of drug
abuse for the last few
decades posing significant
social and health risks.
In a health survey on
drug abuse in 1993,
there were three million
drug users in the country,
with an estimated growth
rate of 6.4% per year.
[6] In 2004 nearly five
million IDUs were there
in Pakistan. [7]
According to the recent
studies there is an
increasing shift from
oral route and inhalation
to injectable drugs
use among addicts, which
is quite alarming.[8]
Studies in countries
like, Russia, Ukraine
and India have shown
that the increasing
scales of injectable
drug use puts a large
group of individuals
at risk of blood born
infections through high
risk behaviors such
as sharing of syringes,
shooting drugs in groups,
low use of condoms and
indulging in commercial
sex. [9] The population
of drug abusers has
been associated with
epidemics of STIs specially
HIV. Sexually transmitted
infections were associated
with use of contaminated
equipment for injecting
drugs and unsafe sex.
There is a body of evidence
supporting the close
association between
drug use and STIs. [10]
These
can
be
divided
into
two
categories.
Commercial
Sex
Contacts
(CCs)
and
Non-Commercial
Sex
Contacts.
In
Pakistan,
CCs
includes
men,
women,
gays,
lesbians,
young
boys
and
hijars.
They
indulge
in
all
types
of
sexual
activities
like
oral,
vaginal
sex
and
anal
sex.
Hijars
are
the
most
common
CCs
for
youth.
They
pose
real
threats
to
youth
because
they
are
cheap
and
easily
accessible.
They
roam
about
on
the
streets
and
roads
of
local
communities
in
groups
and
seduce
young
boys.
It
has
been
observed
many
of
them
suffer
from
anal
gonorrhoea
and
syphilis.
Both
male,
female
and
hijars
work
on
a
daily
basis.
They
usually
go
for
this
work
twice
daily
with
different
partners
and
up
to
five
or
six
on
weekends.
The
most
dangerous
thing
about
them
is
that
they
hide
their
STIs
and
usually
avoid
taking
treatment
unless
they
are
quite
ill.
Mostly
their
clients
include
truck
drivers,
taxi
drivers
and
young
students.
The outcome of STIs is
further aggravated by
their potential to facilitate
the spread of HIV infection.
The presence of HIV/AIDS
also increases the risk
of acquiring other STIs.
It is therefore very important
to bring about the functional
integration of services
for STIs and HIV/AIDS
for achieving better outcomes.
The best intervention
for controlling either
STIs or HIV remains condoms.
STI management centers
can also serve as portals
for condom delivery and
for sexual risk counseling.
STIs
are
transmitted
mainly
due
to
unprotected
sexual
contacts,
vaginal,
anal
or
oral
sex.
Among
the
types
of
sexual
contact,
anal
sex
is
particularly
important.
Due
to
the
trauma
involved
in
an
anal
sex
act,
there
is
more
inflammation
and
this
leads
to
more
acquisition
of
STIs
particularly
HIV.
In
this
regard
promotion
of
condom
use
is
the
most
effective
prevention
strategy
followed
by
reduction
in
partners.
Sexual
and
drug
use
risk
behaviors
of
truck
drivers
/
taxi
drivers
and
their
commercial
sex
contacts
(CCs)
have
been
associated
with
the
spread
of
sexually
transmitted
infections
(STIs)
in
the
developing
world.
A
large
proportion
of
the
truck
drivers
in
Pakistan
are
young
and
are
involved
in
unsafe
sex
with
their
commercial
sex
contacts.
Their
CCs
include
women,
men,
hijars
and
even
very
young
boys.
The
women
and
men
are
mostly
not
trained
in
safe
sex
education.
| WHY
STIs
ARE
INCREASING
IN
PAKISTAN
|
1)
Lack
of
opportunities
of
healthy
sports
and
excursions
for
youth.
2)
Increasing
frustration
in
youth
due
to
easy
access
to
pornographic
material
on
internet
3)
Increasing
influx
of
hijars
from
other
areas
in
local
communities
4)
Increasing
number
of
easily
accessible
new
Female
Sex
Workers
(
FSW)
and
Male
Sex
Workers
(MSW)
5)
Increase
in
the
number
of
Injection
Drug
Users
(IUDs)
| CARE
SEEKING
FOR
STI
SYMPTOMS
IN
PAKISTAN
|
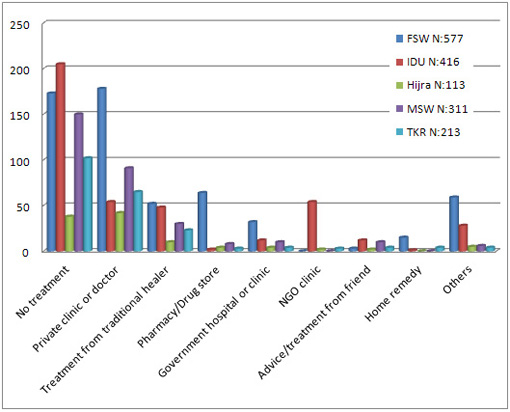
Care
seeking
for
STIs
in
Pakistan
is
similar
to
much
of
other
care
seeking
in
Pakistan.
Most
high
risk
group
members
seek
care
from
the
private
sector
-
mainly
general
practitioners
and
non
medical
personnel.
Public
sector
STI
facilities
tend
to
provide
services
to
mainly
clients
of
sex
workers
and
others
who
acquire
STIs
from
non
commercial
sex.
Adan
Khan
and
associates
conducted
a
survey
to
identify
care
seeking
behavior
of
STIs
patients
[11].
The
author
has
worked
out
a
graph
based
on
their
study.
Please
see
below:
The
National
Guidelines
for
the
Management
of
Sexually
Transmitted
Infections
[12]
suggest
syndromic
management
techniques
because
these
are
cost
effective
and
more
efficacious.
The
six
major
symptom
syndromes:
Urethral
Discharge,
Genital
Ulcer,
Scrotal
Swelling,
Vaginal
Discharge,
Lower
abdominal
pain
and
Anal
symptoms.
| THE
4
C's
MANAGEMENT
STRATEGY
|
The
4Cs
strategy
is
promising
to
improve
treatment
results
and
prevention.
These
include
Compliance,
Counseling,
Condoms
and
Contact
(Partner)
Management.
The
best
prevention
strategy
is
to
avoid
or
reduce
extramarital
sexual
contacts,
partner
reduction
and
use
of
condoms.
Risk
behavior
reduction,
community
based
counseling
and
condom
promotion
are
vital
components
of
these
prevention
programmes.
Family
physicians
provide
the
best
place
for
all
these
tools.
There
must
be
record
keeping
of
patients
suffering
from
STIs.
Partner
notification
can
reduce
the
spread
of
infections.
Treatment
should
follow
the
national
guidelines
and
difficult
to
treat
patients
should
be
referred
to
proper
secondary
and
tertiary
management
centers.
The
management
programmes
must
have
linkages
with
reproductive
health
programmes.
| DRUG
RESISTANCE
IN
STIs
TREATMENT
|
The
drug
resistance
is
emerging
very
rapidly.
Most
of
the
recommended
drugs
show
resistance
even
in
large
doses.
Recurrence
of
infections
is
common.
Patients
are
being
treated
with
a
combination
of
drugs.
This
problem
can
only
be
addressed
if
patients
observe
full
compliance
to
medications.
| FALSE
POSITIVE
SCREENING
TESTS
|
The
commonly
used
VDRL
screening
test
gives
many
false
positive
tests.
This
has
intense
social
implications.
All
recruiting
agencies
for
overseas
employment
do
it
for
all
applicants.
The
false
positive
VDRL
is
ruining
lives
of
especially
female
applicants
as
everyone
hastily
labels
them
corrupt.
There
is
a
rapid
rise
in
STIs
in
Pakistan.
The
rise
in
IUDs
also
poses
a
continued
threat
to
youth.
The
sufferers
prefer
family
physicians
for
advice
and
treatment
because
they
are
easily
accessible
in
their
own
local
communities.
There
is
intense
need
to
train
family
physicians
in
the
prevention,
control
and
treatment
of
STIs.
There
should
be
counseling
facilities
at
all
family
clinics.
There
is
an
urgent
need
for
record
keeping
of
patients
suffering
from
STIs
and
partner
notification.
The
best
way
to
avoid
STIs
is
restriction
to
one
partner,
use
of
condoms
and
reduction
in
number
of
IUDs.
1:
Faiz
NR,
Malik
L,
Raziq
F
et
al.
Frequency
of
vaginal
discharge
and
its
association
with
various
sexually
transmitted
diseases
in
women
attending
antenatal
clinic.
J
Postgrad
Med
Institute
2005;
19:
86-95.
2:
Hashwani
S,
Hinan
T,
Fatima
M.
Awareness
of
sexually
transmitted
diseases
in
a
selected
SAMPLE
in
Karachi.
J
Pak
Med
Assoc
1999;
49:
161-4.
3:
Adler
MW.
Sexually
transmitted
diseases
control
in
developing
countries.
Gentiourin
Med
1996;
72:
83-8.
4:
Atiq
A,
Ansari
FM,
Valente
I.
STI
data.
Pakistan
country
profile.
UNAIDS,
Islamabad,
2002
;
1-26.
5:
Khan
NH,
Hussain
K,
Kanjee
SA,
Wahid
Z.
Reproductive
tract
infections:
a
manual
for
physicians,
reproductive
health.
JCPSP
2002;
12:
150-8.
6:
Farooq
S,
Akhtar
J,
Azeemi
H.
Socio-demographic
and
clinical
characteristics
of
IV
drug
users
presenting
to
tertiary
care
TREATMENT
CENTER.
JPMA
2006;
20:
3-7.
7:
Drug
abuse
in
Pakistan:
Results
from
the
2000
national
assessment.
Anti
Narcotic
force,
Government
of
Pakistan
supported
by
United
Nations
office
for
drug
control
and
crime
prevention,
2002
8:
Shah
SA,
Altaf
A.
Prevention
and
control
of
HIV/AIDS
among
intravenous
drug
users
in
Pakistan:
a
great
challenge.
JPMA
2005;
54:
38-42.
9:
Altaf
A,
Shah
SA,
Memon
A.
Follow
up
study
to
assess
and
evaluate
knowledge,
attitude
and
high-risk
behaviors
and
prevalence
of
HIV,
HBV,
HCV
and
syphilis
among
IDUS
at
Burns
Road,
Karachi.
2003;
External
report
submitted
to
UNODC
10:
Farooq
S,
Akhtar
J,
Azeemi
H.
Socio-demographic
and
clinical
characteristics
of
IV
drug
users
presenting
to
tertiary
care
TREATMENT
CENTER.
JPMA
2006;
20:
3-7.
11:
(JPMA
59:628;
2009).
September,
2009,
Journal
of
Pakistan
Medical
Association,
available
at
http://www.jpma.org.pk/full_article_text.php?article_id=1803
12:
The
National
AIDS
Control
Programme
(Pakistan)
and
The
World
Health
Organization
(WHO)
have
devised
these
guidelines
for
Pakistan.
2007.
|
|
.................................................................................................................

|
| |
|
