|
Prevalence and determinants
of Unintended Pregnancy: Systematic Review
Sumera Aziz
Ali (1)
Shiyam Sunder Tikmani (2)
Waris Qidwai (3)
(1) Senior Instructor, Department of Community
Health Sciences Aga Khan University.
Karachi, Pakistan
(2) Instructor, Research, Community Health Sciences,
Aga Khan University,
Karachi, Pakistan
(3) Professor and Chairman, Family Medicine
Department, Aga Khan University,
Karachi Pakistan
Correspondence:
Dr. Waris Qidwai
Professor and Chairman,
Family Medicine Department
Aga Khan University Karachi Pakistan
Tel: (92-21) 486-4843, 486-4814
Fax: (92-21) 493-4294, 493-2095
Email: waris.qidwai@aku.edu
|
Abstract
Background: Unplanned
pregnancy is one of the leading causes
of maternal mortality and morbidity in
the world. The objective of this systematic
review was to synthesize the findings
of various studies regarding prevalence
and determinates of unintended pregnancy.
Data sources: A
range of electronic databases was searched
for studies conducted in developing countries
and published between 1990 and 2015. English-language
publications were searched using relevant
keywords, and reference lists were hand
searched.
Review methods: A
systematic review was carried out for
all the quantitative studies which met
the inclusion criteria. The quality of
selected studies was assessed using Newcastle-Ottawa
Scale.
Results: Twenty-two
papers were included in the review. Average
prevalence of unintended pregnancy was
estimated to be 35% ranging from 13% to
82%. The predictors of unintended pregnancy
were found to be, socio-demographic factors
include women's age, women's education,
parity, birth order and interval, previous
pregnancy intention, age at the time of
marriage, socioeconomic status, marital
status, religion, caste, and ethnicity.
Conclusion: Main
correlates were found to be age, parity,
educational and economic status. This
means that undertaking outreach in poor
countries might be helpful in fulfilling
the needs of Family planning for these
women. Furthermore, community-based distribution
of family planning methods or counseling
should be targeted to the illiterate older
aged women of reproductive age with poor
socioeconomic status.
Key words: unintended
pregnancy, developing countries, prevalence,
predictors, systematic review
|
According to United Nations (UN) estimation,
the world population is going to reach to 8.1
billion by the year 2025. Developing countries
are attributing to 97% of this burden, which
means 75-78 million people are added annually
by developing countries(1). If this addition
persists, the population of developing countries
will increase from 5.9 billion (in 2013) to
8.2 billion (in 2050) and Asia and Africa countries
will contribute 90% of the increase in population(2).
The reason that developing countries will contribute
more towards the world's population is because
of their high birth rate, which in turn is due
to low contraceptive use(2).
Worldwide use of the modern method of contraception
has increased from 54% to 57%; however contraceptive
usage rates vary widely across the world(3).
In developed countries, more than 80% of women
in reproductive age group (15-49 years) use
contraceptives(2), while contraceptive use is
much lower in African (21%) and Asian (67%)
countries(2). The relatively high usage rates
in Asia are driven to a large extent by near
abundant usage in China (85%), Iran (79%), Sri
Lanka (68%), Japan (54%), India (54%), Bhutan
(66 %) and Indonesia (61%). While Pakistan (35%),
Afghanistan (23%), Maldives (35%) and Nepal
(48%) still lag behind(4, 5). Low contraceptive
prevalence rates are directly related to a high
number of unintended pregnancies(4).
Unintended pregnancies are reported to have
been either unwanted (i.e. occurred when no
more children, were desired) or mistimed (occurred
earlier than desired)(6). Out of 210 million
pregnant women, 75 to 80 million women experience
unintended pregnancies, of which approximately
42 to 46 million pregnancies are terminated
annually worldwide (2, 7, 8).
Currently, both developed and developing countries
are facing the problem of unintended pregnancies
(9, 10). Although worldwide, from 1995 to 2008
the rate of unintended pregnancy has declined
by 20%, from 69 to 55 per 1000 women(9, 10).
This decline in the rate of unintended pregnancy
was greater in the developed world, where it
fell by 29 percent (from 59 to 42 per 1000 women);
while it declined by 20 percent, from 71 to
57 per 1000 women in the developing countries(9,
10). The highest rates of unintended pregnancies
were in Africa (86 /1000 women) and the lowest
were in Europe (38/1000 women) (9, 10).
Despite such decline in rates of unintended
pregnancies, its proportion is still high i.e.
about 4 out of 10 pregnancies (40%) were unintended
worldwide in 2008, with a high proportion in
South America and Southern Africa, where 6 out
of 10 pregnancies were unintended(9, 10). It
was even more in developing regions like Latin
America and the Caribbean region (58%), South
Africa (59%), South America (64%) and North
America (48%)(9, 10).
Unplanned pregnancy is one of the leading causes
of maternal mortality and morbidity in South
Asia(6). It is estimated that every year about
one-third of pregnancies are declared unintended
in South and South-East Asia. In 2008, the proportion
of unintended pregnancies in Bangladesh was
30%, while it was 21% in India and 35% in both
Iran(10) and Nepal(1), 46 % both in Yamagata
(Japan) and Pakistan(11, 12). Various reasons
for unintended pregnancies have been identified,
which include non-use of contraceptive methods
and contraceptive method failure(13). Non- use
of contraceptive methods is one of the important
reasons for unintended pregnancy, which is mainly
due to the high unmet need for contraceptives.
Contraceptive method failure incorporates both
users and technological faults(13).
In addition to this, different factors may predict
or determine unintended pregnancy and numerous
studies have reported different predictors of
unintended pregnancies. Although the prevalence
and determinants of unintended pregnancy are
reported from multiple countries through various
studies, however these studies are not compiled
and synthesized particularly both from developed
and developing countries. Thus, the objective
of this systematic review was to synthesize
the findings of various studies regarding prevalence
and determinates of unintended pregnancy.
Eligibility criteria
Eligible studies were those that were cohort
or demographic health surveys, conducted in
low-, middle or high-income countries, reported
the prevalence and risk factors of unintended
pregnancy and reported estimates of the odds
ratio, risk ratio, or relative risk.
Search strategy
Under guidance of the librarian, we searched
a range of electronic bibliographic databases:
Medline and Embase through Ovid (1990 to 2015),
Cochrane Library through Wiley Interscience,
Cumulative Index to Nursing and Allied Health
Literature (CINAHL) through EBSCO Host, PubMed
through the National Center for Biotechnology
Information (NCBI), and SCOPUS through Elsevier.
We used a combination of Medical Subject Headings
keywords, and text words for "unintended
AND pregnancy", "prevalence",
"mistimed", "unwanted",
"risk factors", "predictors",
"determinants" and "correlates"
that appeared in abstracts and titles.
Search outcome
Data abstraction and quality assessment
Two reviewers (Medical doctors) independently
abstracted data from all of the included studies.
Abstracted data included study design; type
of database used for analysis (population-based
or hospital-based) ; characteristics of the
study subjects, unintended pregnancy definition;
potential confounders or effect modifiers considered;
and risk ratio or odds ratio for unintended
pregnancy. We assessed the quality of each study
using the Newcastle-Ottawa Scale(14) for all
studies. Differences in data abstraction were
resolved by consensus between two reviewers.
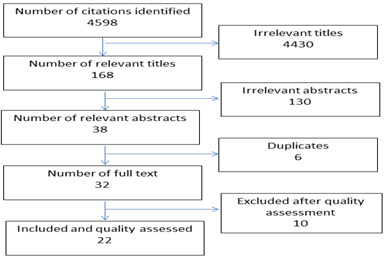
Search
outcome
Of
4598
research
papers
initially
identified
using
the
search
criteria,
4430
articles
were
found
to
be
irrelevant
after
reviewing
the
titles.
The
abstracts
of
the
remaining
168
papers
with
relevant
articles
were
then
examined.
Of
these,
130
abstracts
were
found
to
be
irrelevant.
Thus,
full
papers
of
the
remaining
38
abstracts
were
accessed
and
6
were
found
to
be
duplicates.
Finally,
32
full
papers
were
assessed
for
quality
and
eligibility.
Thus,
22
unique
citations
were
identified
which
met
the
inclusion
criteria
(Figure
1).
The
characteristics
of
the
individual
studies
are
summarized
in
Table
1.
Those
studies
which
were
conducted
from
1990
to
2015
were
retrieved
for
this
review.
Studies
varied
with
regard
to
criteria
for
defining
unintended
pregnancy.
Some
of
the
studies
had
assessed
the
intention
through
binary
outcome
(intended
or
unintended)
while
others
had
assessed
the
intention
under
three
categories
(mistimed,
wanted
and
unwanted).
All
studies
were
quantitative
and
among
the
selected
studies,
8
analyzed
secondary
data
from
demographic
health
surveys
or
other
national
health
surveys,
while
14
were
primary
studies
including
12
cross-sectional
studies
and
2
cohort
studies.
Of
the
22
studies,
18
had
measured
the
prevalence
of
unintended
pregnancy
and
22
had
measured
the
determinants
of
unintended
pregnancy.
Of
these
22
studies,
11
were
from
Africa,
9
from
Asia,
1
each
from
Europe
and
North
America.
All
the
determinants
were
categorized
into
three
themes
i.e.
Socio-demographic
factors,
Affordability
and
women's
knowledge,
attitudes,
beliefs
and
culture.
Prevalence
of
Unintended
pregnancy
Of
the
18
studies
which
had
measured
the
prevalence
of
unintended
pregnancy,
it
was
found
that
average
prevalence
was
estimated
to
be
35%
ranging
from
13%
to
82%.
Factors
determining
the
unintended
pregnancy
Socio-demographic
factors
Socio-demographic
factors
included
women's
age,
women's
education,
parity,
birth
order
and
interval,
previous
pregnancy
intention,
age
at
the
time
of
marriage,
socioeconomic
status,
marital
status,
religion,
caste,
and
ethnicity.
Thirteen
studies
found
that
women's
age
was
the
best
predictor
of
pregnancy
intention
(Table
1).
Of
these,
8
studies
showed
that
older
women
were
more
likely
to
experience
unintended
pregnancy
(15-21)
while
five
studies
had
shown
that
younger
women
were
at
risk
of
unintended
pregnancy
(17,
21-24).
Seven
studies
found
that
women's
education
was
the
best
predictor
of
pregnancy
intention
(Table
1).
Of
these,
5
studies
showed
that
women
with
primary
or
less
education
were
more
likely
to
experience
unintended
pregnancy
(17,
19,
25-27)
while
two
studies
had
shown
contradictory
findings(20,
26).
Ten
studies
found
strong
associations
between
parity
and
pregnancy
intention
(Table
1).
Among
all
the
studies,
higher
parity
was
generally
found
to
be
the
positive
predictor
of
unintended
pregnancy.
In
addition
to
this,
four
studies
found
strong
associations
between
age
at
the
time
of
marriage
and
pregnancy
intention
(Table
1).
All
the
studies
had
shown
the
inverse
relation
between
age
at
the
time
of
marriage
and
pregnancy
intention,
as
the
age
at
the
time
of
marriage
increased,
the
likelihood
of
unintended
pregnancy
reduced
(20,
28-30)
.
Likewise,
five
studies
showed
that
religion
played
a
significant
role
for
the
pregnancy
intention.
Around
60%
of
these
studies
found
that
non-Muslims
were
less
likely
to
experience
unintended
pregnancy
as
compared
to
Muslims
while
40%
had
shown
the
opposite
findings(17,
31).
Seven
studies
found
strong
associations
between
marital
status
and
pregnancy
intention
(Table
1).
Of
these,
four
studies
found
that
married
women
were
less
likely
to
experience
unintended
pregnancy
as
compared
to
unmarried
women.
Three
studies
found
that
married
women
were
more
at
risk
of
experiencing
unintended
pregnancy
(Table
1).
Affordability
Eight
studies
found
significant
relationships
between
economic
factors
(socio-economic
status
or
income
of
the
household,
working
status
of
woman
and
woman's
employment)
and
pregnancy
intention
(20,
28-30).
The
financial
constraint
was
the
most
important
factor
determining
the
intention
of
pregnancy.
Generally,
women
with
high
economic
status
were
less
likely
to
experience
unintended
pregnancy
except
the
one
study,
which
contradicted
the
above
findings.
Women's
knowledge,
attitudes,
beliefs,
and
culture
Different
variables
were
included
under
this
category
like
access
to
media,
knowledge
and
practice
of
Family
planning
methods.
Only
one
study
from
Nepal
showed
that
exposure
to
mass
media
(radio)
significantly
predicted
pregnancy
intention
(Table
1).
Women
with
high
levels
of
exposure
were
less
likely
to
experience
unintended
pregnancy(28).
Four
studies
had
found
the
strong
association
between
pregnancy
intention
and
knowledge
of
Family
planning
methods
(Table
1).
Of
these
4
studies,
50%
had
shown
that
knowledge
was
positively
associated
with
pregnancy
intention
and
50%
of
these
had
shown
the
negative
association
between
two
variables(28,
32).
Additionally,
eight
studies
had
shown
that
contraceptive
usage
had
also
shown
significant
association
with
unintended
pregnancy,
6
studies
found
the
positive
association
with
unintended
pregnancy
while
2
studies
found
the
negative
association.
Click
here
for
Table
1:
Prevalence
and
determinants
of
unintended
pregnancy
Click
here
for
Table
2:
Quality
assessment*
of
individual
studies
included
in
the
systematic
review
Figure
1:
Flow
diagram
showing
the
process
of
retrieving
the
articles
FLOW
CHART
This
review
has
evaluated
all
the
peer-reviewed
studies,
published
in
English
language
from
1990-2015.
It
was
found
that
the
prevalence
of
unintended
pregnancy
ranged
from
13-82%.
Common
predictors
identified
were
age,
parity,
socioeconomic
status,
religion
and
use
of
family
planning
methods.
Age
was
found
to
be
positively
associated
with
unintended
pregnancy
in
most
of
the
studies.
Studies
from
Bangladesh,
Ethiopia,
Egypt,
Nepal,
Spain,
Vietnam
and
Nigeria
reported
the
positive
association
of
age
with
an
unintended
pregnancy
(16,
21,
23,
27,
28,
33,
34).
Consistent
with
definitions
of
mistimed
and
unwanted
pregnancies,
this
review
showed
that
mistimed
pregnancies
occurred
to
younger
women
and
were
seen
more
often
in
the
first
and
second
pregnancies,
while
unwanted
pregnancies
occurred
to
older
women
and
in
the
third
or
later
pregnancies.
Furthermore,
this
analysis
showed
that
many
mistimed
and
unwanted
pregnancies
occurred
either
as
a
result
of
no
contraceptive
use,
or
due
to
method
failure.
Although
we
could
not
explore
the
types
of
methods
used
by
the
women
or
reasons
for
method
failure,
the
increased
likelihood
of
unintended
pregnancy
among
users
of
contraceptive
methods
could
be
due
to
inappropriate
usage
of
short
term
methods,
which
has
been
highlighted
through
prior
research(35).
Studies
from
Kenya,
Ethiopia,
Ghana,
Tanzania
and
Bangladesh
reported
that
high
parity
was
significantly
associated
with
unintended
pregnancy
(22,
23,
31-33).
These
findings
can
be
explained
by
the
fact
that
couples
from
rural
areas
prefer
to
have
more
sons
and
they
may
end
up
having
more
children.
Furthermore,
women
in
the
Asian
region
usually
prefer
to
have
enough
sons
who
can
become
their
source
of
income
for
the
family(34).
Moreover,
these
couples
want
to
balance
the
sex
of
their
children,
and
will
continue
to
give
birth
if
all
the
children
are
of
the
same
sex.
In
this
review,
it
was
found
that
wealth
quintile
and
educational
status
was
associated
with
unintended
pregnancy
in
the
same
direction.
Studies
from
Ethiopia,
Japan,
Spain,
Bangladesh
and
Nigeria
reported
that
illiterate
women
or
women
with
primary
education
are
at
risk
of
unintended
pregnancy
(17,
23,
26,
27,
33).
This
finding
can
be
explained
by
the
fact
that
women
may
not
even
realize
that
they
are
pregnant
until
it
has
become
too
late,
and
they
may
not
be
able
to
negotiate
with
their
spouses
with
regards
to
safe
sex.
Knowledge
about
contraceptives
was
reported
to
be
negatively
associated
with
unintended
pregnancy(17,
28).
Various
studies
found
that
women
who
have
more
knowledge
about
contraceptives
are
less
likely
to
experience
an
unintended
pregnancy,
as
compared
to
those
who
do
not
have
adequate
knowledge
about
these
methods.
Moreover,
the
use
of
contraceptive
methods
is
positively
associated
with
unintended
pregnancy.
Studies
have
also
found
a
strong
positive
association
between
users
of
modern
contraceptives
and
unintended
pregnancy,
which
can
be
explained
by
the
fact
that
users
of
these
methods
might
fail.
Since
this
review
did
not
focus
on
method
failure,
therefore,
it
can
be
assumed
that
method
failure
might
have
increased
the
chances
of
unintended
pregnancy
among
these
women.
With
respect
to
women's
autonomy,
men
are
usually
considered
as
the
main
decision-makers
in
developing
countries,
and
they
decide
when
and
where
a
woman
should
seek
healthcare.
Hence,
women
are
often
given
less
power
in
the
male-dominant
societies
to
decide
for
themselves,
and
they
have
to
depend
on
the
male
partners/relatives
for
their
survival
and
other
life
matters.
Besides,
social
norms
limit
women's
freedom
to
make
important
decisions(36).
In
some
regions
of
South
Asia,
women
have
substantially
lower
social
status
and
autonomy
than
men(37).
It
has
been
found
that
low
social
status
and
autonomy
seems
to
be
associated
with
low
fertility
control(38).
Such
women
are
more
likely
to
experience
an
unintended
pregnancy,
as
compared
to
those
who
have
some
autonomy(36).
Strengths
and
Limitations
of
the
Study
We
believe
that
this
is
first
systematic
review
on
prevalence
and
predictors
of
unintended
pregnancy,
which
has
synthesized
the
data
both
from
developing
and
developed
countries.
Despite
the
extensive
literature
review,
there
are
some
limitations
to
this
study.
Firstly,
we
had
reviewed
all
the
cross-sectional
studies
except
one
cohort
study,
therefore
causal
association
between
various
determinants
and
unintended
pregnancy
cannot
be
determined
to
establish
a
relationship
between
unintended
pregnancy
and
various
studied
correlates.
Secondly,
different
countries
have
different
predictors
for
unintended
pregnancy,
depending
upon
the
epidemiologic
and
demographic
variations
in
those
particular
countries,
so
results
might
not
be
generalized
to
all
settings.
Thirdly,
this
review
included
papers
only
in
the
English
language
and
we
might
have
missed
the
important
information
published
in
language
other
than
English.
The
decision
to
exclude
non-English
language
studies
was
made
for
practical
reasons
based
on
the
increased
time,
expense
and
complexity
of
translating
and
synthesizing
these
studies.
However,
much
research
in
developing
countries
may
not
be
published
in
peer-reviewed
journals,
but
might
be
available
as
gray
literature
in
local
languages.
These
limitations
should
have
a
minor
impact
on
the
scope
of
the
study
in
view
of
the
large
size
of
the
sample
and
that
the
main
variables
of
interest
are
demographic
factors
associated
with
unintended
pregnancy.
| CONCLUSION
AND
RECOMMENDATIONS
|
This
review
demonstrates
that
unintended
pregnancy
is
common
both
in
developing
and
developed
countries
and
age,
parity,
educational
and
economic
status
can
be
considered
as
important
determinants
of
the
unintended
pregnancy.
This
means
undertaking
outreach
in
poor
and
inaccessible
settings
and
providing
community-based
distribution
of
family
planning
methods
including
counseling
and
referral
for
women
with
unmet
need.
In
addition
to
this,
programs
can
be
undertaken
to
target
youth
through
youth
corners
in
existing
health
facilities
or
training
providers
in
offering
youth
friendly
services.
Implementation
of
targeted
programs
will
guarantee
access
to
family
planning
for
all
categories
of
women
in
need.
These
types
of
targeted
approaches
can
help
women
to
meet
their
fertility
desires
and
reduce
unintended
pregnancies
with
the
overall
objective
of
reducing
maternal
mortality
and
morbidity.
1.
Haub
C,
Gribble
J,
Jacobsen
L.
World
Population
Data
Sheet
2011.
Population
Reference
Bureau,
Washington.
2011.
2.
Hossain
SMI,
Khan
M,
Rahman
M,
Sebastian
MP.
South
east
Asia
regional
training
manual.
New
Delhi,
India:
Population
Council.
2005.
3.
Press
B.
Round
Up.
Reproductive
Health
Matters.
2010;18(35):211-8.
4.
Ali
SA,
Ali
SA.
Unmet
need
for
contraception
and
unintended
pregnancies
among
women
of
reproductive
age
group:
A
situation
analysis.
Elective
Medicine
Journal.
2014;2(3):259.
5.
Tsui
AO,
McDonald-Mosley
R,
Burke
AE.
Family
planning
and
the
burden
of
unintended
pregnancies.
Epidemiologic
reviews.
2010:mxq012.
6.
Smith
R,
Ashford
L,
Gribble
J,
Clifton
D.
Family
planning
saves
lives.
2009.
7.
Glasier
A,
Gülmezoglu
AM,
Schmid
GP,
Moreno
CG,
Van
Look
PF.
Sexual
and
reproductive
health:
a
matter
of
life
and
death.
The
Lancet.
2006;368(9547):1595-607.
8.
Kott
A.
Rates
of
unintended
pregnancy
remain
high
in
developing
regions.
International
perspectives
on
sexual
and
Reproductive
Health.
2011;37(1):46-7.
9.
Singh
S,
Sedgh
G,
Hussain
R.
Unintended
pregnancy:
worldwide
levels,
trends,
and
outcomes.
Studies
in
family
planning.
2010;41(4):241-50.
10.
Abbasi-Shavazi
MJ,
Hosseini-Chavoshi
M.
Unintended
pregnancies
in
the
Islamic
Republic
of
Iran:
levels
and
correlates.
Asia-Pacific
population
journal.
2004;19(1):27-38.
11.
Collumbien
M,
Gerressu
M,
Cleland
J.
Non-use
and
use
of
ineffective
methods
of
contraception.
2004.
12.
Sathar
Z,
Singh
S,
Rashida
G,
Shah
Z,
Niazi
R.
Induced
abortions
and
unintended
pregnancies
in
Pakistan.
Studies
in
family
planning.
2014;45(4):471-91.
13.
Kost
K,
Singh
S,
Vaughan
B,
Trussell
J,
Bankole
A.
Estimates
of
contraceptive
failure
from
the
2002
National
Survey
of
Family
Growth.
Contraception.
2008;77(1):10-21.
14.
Stang
A.
Critical
evaluation
of
the
Newcastle-Ottawa
scale
for
the
assessment
of
the
quality
of
nonrandomized
studies
in
meta-analyses.
European
journal
of
epidemiology.
2010;25(9):603-5.
15.
Ma
Q,
Pan
X,
Cai
G,
Yan
J,
Xu
Y,
Ono-Kihara
M,
et
al.
Unintended
Pregnancy
and
Its
Correlates
among
Female
Attendees
of
Sexually
Transmitted
Disease
Clinics
in
Eastern
China.
BioMed
research
international.
2013;2013.
16.
Youssef
R,
Moubarak
I,
Gaffar
Y,
Atta
H.
Correlates
of
unintended
pregnancy
in
Beheira
governorate,
Egypt.
2002.
17.
Tebekaw
Y,
Aemro
B,
Teller
C.
Prevalence
and
determinants
of
unintended
childbirth
in
Ethiopia.
BMC
pregnancy
and
childbirth.
2014;14(1):1.
18.
Faye
CM,
Speizer
IS,
Fotso
JC,
Corroon
M,
Koumtingue
D.
Unintended
pregnancy:
magnitude
and
correlates
in
six
urban
sites
in
Senegal.
Reproductive
health.
2013;10(1):59.
19.
Islam
MM,
Rashid
M.
Determinants
of
unintended
pregnancy
among
ever-married
women
in
Bangladesh.
Journal
of
Family
Welfare.
2005;50(2):40.
20.
Okonofua
FE,
Odimegwu
C,
Ajabor
H,
Daru
PH,
Johnson
A.
Assessing
the
prevalence
and
determinants
of
unwanted
pregnancy
and
induced
abortion
in
Nigeria.
Studies
in
family
planning.
1999;30(1):67-77.
21.
Sedgh
G,
Bankole
A,
Oye-Adeniran
B,
Adewole
IF,
Singh
S,
Hussain
R.
Unwanted
pregnancy
and
associated
factors
among
Nigerian
women.
International
family
planning
perspectives.
2006:175-84.
22.
Ikamari
L,
Izugbara
C,
Ochako
R.
Prevalence
and
determinants
of
unintended
pregnancy
among
women
in
Nairobi,
Kenya.
BMC
pregnancy
and
childbirth.
2013;13(1):1.
23.
Kamal
M,
Islam
A.
Prevalence
and
socioeconomic
correlates
of
unintented
pregnancy
among
women
in
rural
Bangladesh.
salud
pública
de
méxico.
2011;53(2):108-15.
24.
Besculides
M,
Laraque
F.
Unintended
pregnancy
among
the
urban
poor.
Journal
of
Urban
Health.
2004;81(3):340-8.
25.
Habte
D,
Teklu
S,
Melese
T,
Magafu
MG.
Correlates
of
unintended
pregnancy
in
Ethiopia:
results
from
a
national
survey.
PLoS
One.
2013;8(12):e82987.
26.
Takahashi
S,
Tsuchiya
KJ,
Matsumoto
K,
Suzuki
K,
Mori
N,
Takei
N,
et
al.
Psychosocial
determinants
of
mistimed
and
unwanted
pregnancy:
the
Hamamatsu
Birth
Cohort
(HBC)
study.
Maternal
and
child
health
journal.
2012;16(5):947-55.
27.
Font-Ribera
L,
Pérez
G,
Salvador
J,
Borrell
C.
Socioeconomic
inequalities
in
unintended
pregnancy
and
abortion
decision.
Journal
of
Urban
Health.
2008;85(1):125-35.
28.
Adhikari
R,
Soonthorndhada
K,
Prasartkul
P.
Correlates
of
unintended
pregnancy
among
currently
pregnant
married
women
in
Nepal.
BMC
International
Health
and
Human
Rights.
2009;9(1):1.
29.
Che
Y,
Cleland
J.
Unintended
pregnancy
among
newly
married
couples
in
Shanghai.
International
family
planning
perspectives.
2004:6-11.
30.
Goto
A,
Yasumura
S,
Reich
MR,
Fukao
A.
Factors
associated
with
unintended
pregnancy
in
Yamagata,
Japan.
Social
Science
&
Medicine.
2002;54(7):1065-79.
31.
Exavery
A,
Kanté
AM,
Njozi
M,
Tani
K,
Doctor
HV,
Hingora
A,
et
al.
Predictors
of
mistimed,
and
unwanted
pregnancies
among
women
of
childbearing
age
in
Rufiji,
Kilombero,
and
Ulanga
districts
of
Tanzania.
Reproductive
health.
2014;11(1):63.
32.
Eliason
S,
Baiden
F,
Yankey
BA,
Awusabo-Asare
K.
Determinants
of
unintended
pregnancies
in
rural
Ghana.
BMC
pregnancy
and
childbirth.
2014;14(1):1.
33.
Kassa
N,
Berhane
Y,
Worku
A.
Predictors
of
unintended
pregnancy
in
Kersa,
Eastern
Ethiopia,
2010.
Reprod
Health.
2012;9(1):2-7.
34.
Le
LC,
Magnani
R,
Rice
J,
Speizer
I,
Bertrand
W.
Reassessing
the
level
of
unintended
pregnancy
and
its
correlates
in
Vietnam.
Studies
in
family
planning.
2004:15-26.
35.
Keshtkaran
A.
The
survey
of
effective
factors
on
different
practical
failure
methods
of
family
planning
in
women
referred
to
health
centers.
Middle
East
Journal
of
Family
Medicine.
2005;3(2).
36.
Ali
A,
Ali
SA,
Aziz
Ali
S,
Khuwaja
NS.
Determinants
of
Unintended
Pregnancy
among
Women
of
Reproductive
Age
in
Developing
Countries:
A
Narrative
Review.
Journal
of
Midwifery
and
Reproductive
Health.
2016;4(1):513-21.
37.
Weiner
M.
Sons
of
the
soil:
Migration
and
ethnic
conflict
in
India.
Princeton
University
Press;
2015.
38.
Singh
KK,
Singh
K,
Singh
BP,
Pathak
AK.
Impact
of
education
and
autonomy
on
fertility
of
women
in
eastern
Uttar
Pradesh.
Demography
India.
2015;31(2):223-33.
|

