|
Frequency of Job-Related
Burn-out in Family Physicians working in General
/ Family Practice in the Middle East
Abdulrazak Abyad
(1)
Bader Almustafa (2)
Abbas Ali Mansour (3)
Manal S Al-Mutar (4)
Thamer Al Hilfi (5)
Seyed Habib Olla Kavari (6)
Middle East Primary Care Research Network
Research Project
(1) A. Abyad, MD, MPH, MBA, AGSF, AFCHSE., Lebanon,
(2) Bader Almustafa, MD. Saudi Arabia
(3) Abbas Ali Mansour, MD, Iraq
(4) Manal S Al-Mutar, MD, Kuwait
(5) Thamer Al Hilfi, MD, Iraq
(6) Seyed Habib Olla Kavari, Iran
Correspondence:
A. Abyad, MD, MPH, MBA, AGSF, AFCHSE.,
Tripoli
Lebanon
Email: aabyad@cyberia.net.lb
|
Abstract
Introduction: The
aim of this study was to determine the
prevalence of burnout, and of asso- ciated
factors, amongst family doctors (FDs)
in the Middle East.
Methodology:A
cross-sectional survey of FDs was conducted
using a custom-designed and validated
questionnaire which incorporated the Maslach
Burnout Inventory Human Services Survey
(MBI-HSS) as well as questions about demographic
factors, working experience, health, lifestyle
and job satisfaction. MBI-HSS scores were
analysed in the three dimensions of emotional
exhaustion (EE), depersonalization (DP)
and personal accomplishment (PA).
Results: Seven
hundred questionnaires were distributed
in 5 Midlde Eastern countries, and 500
were returned to give a response rate
of 71%. As far as burnout, 44% of respondents
scored high for EE burnout, 30% for DP
and 28% for PA, with 15% scoring high
burnout in each of the three measurements.
A little more than 33% of doctors did
not score high for burnout in any dimesnion.
High burnout was observed to be emphatically
connected with a few of the variables
under concentrate, particularly those
relative to respondents' nation of home,
occupation fulfillment, expectation to
change work, sick leave usage, the misuse
of liquor, tobacco and psychotropic medication,
more youthful age and male sex.
Conclusions: Burnout
is by all accounts a typical issue in
FDs over the Midlde East and is connected
with individual and workload pointers,
and particularly work fulfillment, aim
to change work and the abuse of liquor,
tobacco and medicine. The study survey
has all the earmarks of being a substantial
instrument to quantify burnout in FDs.
Proposals for changes of employment conditions
and future research are needed for further
exploring the issue.
Key words:
Burnout, Middle East, general practice,
job satisfaction.
|
The practice of medicine is inherently stressful.
Physicians must continuously respond to the
needs of patients and their families, routinely
interact with the most intense emotional aspects
of life and expend their own emotional resources
to provide care and caring to others. Each day,
physicians are called on to cope and adapt with
stresses characteristic of their role. Extensive
'withdrawals' from emotional reserves are required,
while emotional 'deposits' may be infrequent
and few. For some, each day becomes increasingly
more difficult as coping mechanisms prove inadequate
and emotional reserves become depleted (1).
Burnout is generally characterized as loss
of eagerness for work, sentiments of negativity,
and a low feeling of individual achievement.
There have been inquiries concerning the utilization
of these criteria, in any case. Burnout is a
reaction to chronic, job-related stress. It
is an emotional state that may be accompanied
by a number of physical and behavioural changes.
It is a construct used to describe negative
changes in the attitudes, moods, and behaviours
of individuals in reaction to stresses at work.
The sources of burnout in physicians are maladaptive
coping habits, which are fostered by the medical
training system. Postgraduate training in medicine
involves long hours, excessive workloads, sleep
deprivation, changing working conditions, peer
competition, self-denial, and social isolation
from the 'real world' (2).
Those physicians who manage to survive their
training years find that their expectations
often do not conform to reality. Instead of
the ideal life they envisioned, they find numerous
new sources of stress waiting for them. Many
arrive at this point with their sense of self-worth
completely tied to their productivity. A growing
practice would seem to be a sign of success
and gratification but may actually require a
physician having to work faster and longer to
meet demands. Under these conditions, the practice
may become routine and tedious. The rapidly
increasing body of medical knowledge and technology
make it difficult to keep up to date, and there
is an increasing pressure to focus on the disease
rather than the patient (3).
It is estimated that between 30-40% of physicians
suffer from burnout at a level sufficient to
affect their personal or professional performance.
Prevalence rates for depression and stress (anxiety
and burnout) have been reported for British
general practitioners, Canadian and American
emergency room physicians, American Internists,
American family practice residents, Spanish
and Canadian general practitioners (4).
A national overview distributed in the Archives
of Internal Medicine in 2012 reported that US
doctors endure more burnout than other American
workers (5). This year, in the Medscape Physician
Lifestyle Report, 46% of all doctors reacted
that they had burnout, which is a generous increment
since the Medscape 2013 Lifestyle Report, in
which burnout was accounted for in marginally
under 40% of respondents.. A few studies have
recommended that a low feeling of individual
achievement is not connected with burnout, in
any event in men (6,7).
In other studies , essentially including the
statements "I feel burned out from my work"
and "I have become more callous toward
people since I took this job" appears to
be a valid method for measuring burnout (8,
9). Given the vagueness in characterizing and
measuring burnout, the criteria utilized as
a part of the Medscape review to survey burnout
in our doctor individuals give helpful data
on the present condition of doctor morale which,
tragically, is low.
An article distributed in the Journal of General
Internal Medicine reported burnout rates running
from 30% to 65% across specialties, with the
most elevated rates brought about by doctors
at the front of care, such as, emergency medicine
and primary care (10). The 2015 Medscape study
results mirror this same example, with the most
elevated burnout rates found in critical care
(53%) and emergency medicine (52%), and with
half of all family doctors, internists, and
general surgeons reporting burnout. Of considerably
more worry, among internists and family doctors
who reacted to the Medscape overview, burnout
rates ascended from around 43% in 2013 to half
in both gatherings, a flat out expansion of
7% however a 16% ascent in frequency in only
2 years. In a year ago's Medscape Physician
Compensation Report, family doctors and internists
were two of the specialties most likely to say
they would choose medicine again, but also two
of the specialties most likely to say they would
not choose their own specialty again.
Other studies have demonstrated that the pervasiveness
of burnout in essential consideration doctors
(PCPs) has expanded over the earlier decade
in the United States as well as in Europe (7,11).
The minimum worn out doctors as indicated by
our study are dermatologists (37%), therapists
(38%), and pathologists (39%). As far as we
can tell no one has yet documented rates of
burnout in general practice in the Middle East.
Burnout can be prevented by psychological or
social interventions. The aim of this study
is to quantify burnout in Middle-Eastern FPs/GPs
(Family Doctors/General Practitioners), and
try to identify factors which predict burnout
in the study population.
Objectives
The objective of this study is to perform a
survey of burnout in General Practice/Family
Medicine, with the participation of Middle-Eastern
FPs/GPs. We may then investigate the frequency
of burnout in FPs/GPs and to identify risk factors
contributing to the development of such burnout.
| STUDY
POPULATION
-
METHODS
-
RESEARCH
PLAN |
Randomly
assigned
FPs/GPs
from
participant
countries
wereasked
to
participate
in
this
study.
The
randomisation
and
sample
selection
process
was
co-ordinated
by
a
key
FP/GP
in
each
Country,
selected
from
the
participants
of
project
meeting,
or
their
delegates.
Each
Country
was
expected
to
provide
up
to
100
completed
questionnaires
to
the
co-ordinating
doctors
(authors)
for
analysis.
Participating
doctors
were
asked
to
complete
a
questionnaire
that
had
two
parts
,
and
which
had
been
piloted
successfully
and
validated
(12)
(Table
1):
Click
here
for
Table
1
(pdf)
Part
one
was
a
self-prepared
questionnaire
with
questions
about
demographic
information,
with
questions
on
working
place,
working
tenure,
training,
workload,
remuneration,
job
satisfaction,
alcohol
consumption,
smoking,
use
of
psychoactive
medication,
sick
leave,
etc.
Part
two
was
the
Maslach
Burnout
Inventory,
Human
Services
Survey,
a
conceptualization
of
burnout
as
a
syndrome
characterized
by
three
dimensions:
emotional
exhaustion,
depersonalization
and
decreased
sense
of
personal
accomplishment
(13),
and
Part
three
was
a
seven-point
Likert
type
satisfication
questionnaire.
In
those
Countries
where
the
use
of
an
English-language
instrument
may
have
posed
a
barrier,
the
questionnaire
was
translated
to
the
native
language
by
the
key
co-ordinating
FP/GP
in
that
Country.
The
translation
process
was
validated
by
cross
translation.
| DATA
COLLECTION
AND
STATISTICAL
ANALYSIS
|
The
country
co-ordinators,
one
lead
FD
in
each
of
5
participating
countries
were
responsible
to
send
the
questionnaire
to
a
representative
sample
of
their
country's
FDs.
The
original
target
was
a
sample
size
of
100
completed
questionnaires
from
each
country.
Each
country
co-ordinator
coded
the
data
from
the
returned
questionnaires
into
a
custom-
designed
Microsoft
Excel
spreadsheet
template,
and
these
were
then
imported
into
SPSS
version
17
by
the
coordinator
of
the
study
.
Scores
were
output
in
the
three
dimensions
of
burnout
and
were
then
transformed
into
dummy
categorical
variables
for
high,
average
and
low
burnout
in
the
dimensions
of
emotional
exhausation
(EE),
depersonalization(DP),
and
Personal
Accomplishment
(PA)
as
recommended
by
Maslach
using
the
cutoff
values
applicable
for
doctors
(13).
However,
the
burnout
outcome
variables
were
recoded
into
high
and
not-high
(average
or
low
burnout)
for
the
statistical
analyses.
EE:
low
burnout
<
13,
average
burnout
14-26,
high
burnout
>
27
(The
scoring
guide
actually
recommends
that
average
scores
for
EE
range
from
19
to
26.
Scores
in
the
range
from
14
to
18
are
thus
difficult
to
classify.
For
the
purposes
of
the
description
of
rates
of
burnout
found
in
this
study,
EE
scores
in
the
range
of
14
to
18
were
classified
as
average,
to
avoid
unclassified
cases.
However,
all
the
statistical
analyses
performed
on
the
data
set
used
the
outcome
variable
of
high
as
against
not
high
burnout
in
the
three
dimensions.)
DP:
low
burnout
<
5,
average
burnout
6-9,
high
burnout
>
10.
PA:
high
burnout
<
33,
average
burnout
34-39,
low
burnout
>
40
(inverse
scale).
A
total
of
500
completed
questionnaires
were
returned
from
more
than
700
sent
giving
a
response
rate
of
approximately
71%.
Among
the
500
respondents
(270
males,
54
%)
had
a
mean
age
of
47.4
years
(SD
6.5
years)
and
had
graduated
15
years
previously
to
filling
in
the
questionnaire
(SD
7.5
years),
worked
42
hours
per
week
(SD
10
hours),
saw
170
patients
per
week
(SD
63
patients)
and
were
roughly
evenly
distributed
amongst
the
5
countries
Table
2:
Job
Satisfication
on
Likert
Scale
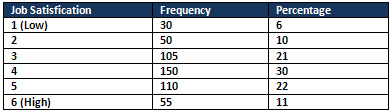
On
the
job
satisfication
questions
on
Likert
scale
6%
of
the
sample
have
very
low
satisfication
and
only
11%
are
highly
satisfied
with
their
jobs.
Table
3
lists
the
frequency
distributions
of
respondents
by
degree
of
burnout
(high,
average
or
low)
in
the
three
dimensions
(EE,
DP,
PA).
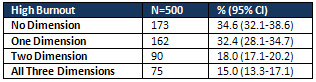
Table
4
gives
the
frequency
distribution
of
respondents
by
presence
of
high
burnout
scores
in
none
(0),
one
or
more
of
the
three
dimensions
(1,
2
or
3).
In
all,
44%
of
respondents
scored
high
for
EE
(95%
CI
=
41.5-45.0%),
30
%
for
high
DP
(28.2-34.9%),
28.0%
low
for
PA
(26.6-32.3%).
In
Table
4
15%
of
respondents
(13.3-17.1%)
scored
high
for
burnout
in
all
three
dimensions.
Only
34.6
%
of
doctors
(32.1-38.6
%)
did
not
score
high
for
burnout
in
any
dimension.
Click
here
for
Table
3:
Frequency
and
cumulative
frequency
distributions
of
respondents
by
degree
of
burnout
(high,
average
and
low)
with
95%
CI
in
each
of
the
three
dimensions
Table
4:
Frequency
and
cumulative
frequency
distributions
of
respondents
by
high
burnout
score
in
none
(0)
or
any
one,
any
two
or
all
three
dimensions
(1,
2
or
3)
with
95%
CI
Iraq
and
Lebanon
scored
the
highest
in
term
burnout
score
in
each
of
the
three
dimensions
followed
by
Iran,
Saudi
Arabia
and
Kuwait.
Lebanese
and
Iranian
respondents
demonstrated
high
proportions
of
high
EE
burnout,
Iraqi
and
Kuwaiti
respondents
demonstrated
high
proportions
of
high
DP
burnout,
whilst
Saudi
respondents
demonstrated
high
proportions
of
high
PA
burnout.
When
looking
at
the
factors
associated
with
high
burnout
the
strongest
associations
using
both
logistic
regression
and
included
job
satisfaction
and
intention
to
change
job,
the
(ab)
use
of
tobacco,
alcohol
and
psychotropic
drugs,
male
sex,
age,
type
of
work
and
sick
leave
utilization.
In
rundown,
MEPCRN
investigation
of
burnout
among
family
doctors
in
5
Middle
Eastern
Countries
with
an
approved
instrument
to
gauge
burnout
accomplished
a
response
rate
of
71%.
Taking
all
things
together,
44%
of
respondents
scored
high
for
EE
burnout,
30%
scored
high
for
DP
burnout
and
28%
scored
high
for
PA
burnout.
Just
34.6%
of
respondents
did
not
score
high
for
burnout
in
any
measurement,
whilst
21%
scored
high
for
burnout
in
no
less
than
two
measurements
and
15%
scored
high
for
each
of
the
three.
In
the
wake
of
controlling
for
nation,
low
occupation
fulfillment,
communicated
goal
to
change
work,
abuse
of
liquor,
tobacco
and
psychotropic
med-ication,
sick
leave
usage,
more
youthful
age,
male
sex
and
kind
of
work
were
connected
with
high
burnout,
as
beforehand
reported.(1)
Some
prior
studies
reported
lower
rates
of
burnout,
yet
a
comparable
number
of
late
studies
reported
comparable
information
(14,15,16,17-21).
Not
surprisingly,
high
burnout
was
more
probable
with
low
occupation
fulfillment
and
goal
to
change
job
(1,
15,22).
Additionally,(1,3,4,14,22)
elevated
amounts
of
burnout
were
observed
to
be
more
probable
with
certain
organizational
elements
(nation
of
root,
as
surrogate
for
health
services
framework,
and
kind
of
work)
and
increased
sick
leave
use,
and
less
so
with
high
workload
(patients
per
week
and
hours
per
week)
and
other
employment
stressors
(pulling
all
nighters
and
weekends).
Individual
variables,
for
example,
more
youthful
age,
sex,
conjugal
status
and
number
of
youngsters
were
likewise
connected
with
burnout,
yet
male
sex
all
the
more
unequivocally
so
(1,22).
Scholastic
work
sort
was
connected
to
lower
EE,
however
higher
PA
burnout,
as
beforehand
reported
(1).
Low
self-regard
has
been
already
answered
to
be
connected
with
burnout.(1)
In
this
study,
we
watched
that
burnout
was
more
probable
with
expanding
smoking,
expanded
utilization
of
liquor
and
utilization
of
psychotropic
drug,
which
might
be
indications
of
low
self-regard
(15).
Different
variables,
for
example,
salary,
were
shockingly
rather
feebly
connected
with
high
burnout,
whilst
others
(non-scholastic
kind
of
work,
years
since
graduation,
not
having
further
capabilities,
expanding
smoking)
appeared
to
be
connected
with
high
EE
burnout,
yet
make
high
PA
burnout
more
outlandish;
be
that
as
it
may,
such
vague
discoveries
have
been
beforehand
depicted
in
burnout
research
in
specialists,
for
instance,
by
Deckard
et
al.
(4)
Generally,
the
example
of
related
variables
seems
like
that
reported
by
Goehring
et
al.(8)
for
those
variables
which
were
incorporated
into
both
studies.
This
is
the
initially
reported
study
exploring
the
pervasiveness
of
burnout
among
Family
Physicians
in
the
Middle
East,
planned
to
look
at
the
variables
connected
with
high
burnout.
The
constraints
of
this
study
incorporate
the
way
that
it
is
cross-sectional,
that
it
has
not
been
led
simultaneously
in
all
nations,
that
the
study
included
FDs
in
different
nations
and
working
in
various
social
insurance
and
healthcare
frameworks
without
measuring
the
multifaceted
nature
of
this
environment.
The
burnout
scores
discovered
seemed
practically
identical
or
high
concerning
prior
studies.
Burnout
is
by
all
accounts
a
typical
issue
in
FDs
crosswise
over
the
Middle
East,
with
high
levels
obviously
influencing
66%
of
respondents
in
this
study.
Taking
all
things
together,
44%
of
respondents
reported
abnormal
amounts
of
EE,
30%
DP
and
28%
low
sentiments
of
PA.
There
is
extensive
variation
between
nations.
High
burnout
was
observed
to
be
more
probable
in
relationship
with
a
few
of
the
variables
under
study,
especially
those
in
respect
to
respondents'
nation
of
living,
work
fulfillment,
intention
to
change
work,
sick
leave
usage,
the
misuse
of
liquor,
tobacco
and
psychotropic
prescription,
younger
age
and
male
sex.
Future
examination
is
expected
to
investigate
the
issue
top
to
bottom,
create
models
to
portray
the
marvel
and
to
recognize
causative
elements
and
compelling
between
intervention
methodologies.
Work
fulfillment
is
an
essential
element
in
such
research,
and
it
ought
to
be
prioritized
by
MEPCRN
as
a
potential
for
further
work
and
research.
Late
research
dealing
with
burnout
expects
to
grow
new
hypothetical
structures
that
expressly
coordinate
both
individual
and
situational
elements,
utilizing
a
model
of
job-person
fit.
Maslach
and
Leiter
(30)
address
the
test
by
defining
a
model
that
spotlights
on
the
degree
of
match
or
befuddle
between
the
individual
and
six
spaces
of
the
employment
environment,
specifically
workload,
control,
reward,
community,
fairness
and
values.
Re-look
has
shown
that
the
more
noteworthy
the
confounder,
the
more
noteworthy
the
potential
for
burnout.
Future
studies
ought
to
address
these
elements
when
examining
burnout
in
FDs,
and
the
attention
ought
to
be
on
positive
as
opposed
to
negative
states,
managing
work
engagement
and
fulfillment
and
not
simply
work
stress.(1)
In
such
manner,
the
solid
relationships
found
in
this
study
between
low
employment
satisfaction
and
burnout
support
the
thought
of
centering
future
examination
on
enhancing
work
fulfillment
instead
of
tending
to
burnout
straightforwardly.
Shockingly,
little
research
has
been
led
into
mediations
for
burnout.
In
spite
of
the
fact
that
examination
demonstrates
that
it
is
the
organizational
attributes
that
appear
to
have
more
grounded
relationship
with
burnout;
generally
intercessions
have
in
the
past
incidentally
been
fixated
on
changing
individuals
(1).
Various
mediation
methodologies
have
been
concentrated,
some
concentrating
on
aversion
of
burnout
and
others
on
treatment
when
it
has
as
of
now
happened,
and
results
have
been
varied
(1).
This
is
another
essential
area
where
our
knowledege
is
lacking.
1.
Deckard
GJ,
Hicks
LL
&
Hamory
BH
(1992).
The
occurrence
and
distribution
of
burnout
among
infectious
disease
physicians.
JID.
165:224-8.
2.
Fawzy
IF,
Fawzy
NW
&
Pasnau
R
(1991).
Burnout
in
the
health
professions.
In:
Handbook
of
studies
on
general
hospital
psychiatry.
Judd,
Burrows,
Lipsitt
(Ed).
NewYork.
Elsevier
Science
Publishers.
pp.119-130.
3.
Deckard
G,
Meterko
M
&
Field
D
(1994).
Physician
Burnout:
An
examination
of
personal,
professional,
and
organisatinal
relationship.
Med
Care.
32:745-754.
4.
Thommasen
HV,
Lavanchy
M,
Connelly
I,
Berkowitz
J.
Mental
health,
job
satisfaction,
and
intention
to
relocate-opinions
of
physicians
in
rural
British
Columbia.
Can
Fam
Physician
2001;47:737-744.
5.
Shanafelt
TD,
Boone
S,
Tan
L,
et
al.
Burnout
and
satisfaction
with
work-life
balance
among
US
physicians
relative
to
the
general
US
population.
Arch
Intern
Med.
2012;172:1377-1385.
http://archinte.jamanetwork.com/article.aspx?articleid=1351351
Accessed
December
1,
2014
6.
Ludwig
DS,
Kabat-Zinn
J.
Mindfulness
in
medicine.
JAMA.
2008;300:1350-1352.
Abstract
7.
Houkes
I,
Winants
Y,
Twellaar
M,
Verdonk
P.
Development
of
burnout
over
time
and
the
causal
order
of
the
three
dimensions
of
burnout
among
male
and
female
GPs.
A
three-wave
panel
study.
BMC
Public
Health.
2011;11:240.
http://www.ncbi.nlm.nih.gov/pmc/articles/PMC3101180/
Accessed
December
3,
2014.
8.
West
CP,
Dyrbye
LN,
Satele
DV,
Sloan
JA,
Shanafelt
TD.
Concurrent
validity
of
single-item
measures
of
emotional
exhaustion
and
depersonalization
in
burnout
assessment.
J
Gen
Intern
Med.
2012;27:1445-1452.
http://link.springer.com/article/10.1007%2Fs11606-012-2015-7
Accessed
December
10,
2014.
9.
Dolan
ED1,
Mohr
D,
Lempa
M,
Joos
S,
Fihn
SD,
Nelson
KM,
Helfrich
CD.
Using
a
single
item
to
measure
burnout
in
primary
care
staff:
a
psychometric
evaluation.
J
Gen
Intern
Med.
2014
Dec
2.
[Epub
ahead
of
print]
10.
Linzer
M,
Levine
R,
Meltzer
D,
Poplau
S,
Warde
C,
West
CP.
10
bold
steps
to
prevent
burnout
in
general
internal
medicine.
J
Gen
Intern
Med.
2014;29:18-20.
http://link.springer.com/article/10.1007/s11606-013-2597-8/fulltext.html
Accessed
December
1,
2014.
11.
Twellaar
M,
Winants
Y,
Houkes
I.
How
healthy
are
Dutch
general
practitioners?
Self-reported
(mental)
health
among
Dutch
general
practitioners.
Eur
J
Gen
Pract.
2008;14:4-9.
Abstract
12.
Yaman
H,
Soler
JK.
The
job
related
burnout
questionnaire.
A
multinational
pilot
study.
Australian
Family
Physician
2002.
31:
1055-6.
13.
Maslach
C.,&
Jackson
S.E.
(1986).
Maslach
Burnout
Inventory.
2nd
ed.
Pal
Alto:
Consulting
Psychologists
Press.
14.
Goehring
C,
Bouvier
Gallacchi
M,
Ku¨
nzi
B,
Bovier
P.
Psychological
and
professional
characteristics
of
burnout
in
Swiss
primary
care
practitioners:
a
cross-sectional
survey.
Swiss
Med
Wkly.
2005;
135:
101-108.
15.
Thommasen
HV,
Lavanchy
M,
Connelly
I,
Berkowitz
J,
Grzybowski
S.
Mental
health,
job
satisfaction
and
intention
to
relocate.
Can
Fam
Physician
2001;
B47:
737-744.
16.
Yaman
H,
Soler
JK.
The
job-related
burnout
questionnaire
in
family
practice:
a
multinational
pilot
study.
Aust
Fam
Physician.
2002;
31:
1055-1056.
17.
Cathebras
P,
Begon
A,
Laporte
S,
Bois
C,
Truchot
D.
Burn
out
among
French
general
practitioners.
Presse
Med.
2004;
33:1569-1574.
18.
Prieto
Albino
L,
Robles
Aguero
E,
Salazar
Martinez
LM,
Daniel
Vega
E.
Burnout
in
primary
care
doctors
of
the
province
of
Ca-
ceres.
Aten
Primaria.
2002;
29:
294-302.
19.
Esteva
M,
Larraz
C,
Jimenez
F.
La
salud
mental
en
los
me`
dicos
de
familia:
efectos
de
la
satisfaccio`
n
y
el
estre`
s
en
el
trabajo.
Rev
Clin
Esp.
2006;
206:
77-83.
20.
Grassi
L,
Magnani
K.
Psychiatric
morbidity
and
burnout
in
the
medical
profession:
an
Italian
study
of
general
practitioners
and
hospital
physicians.
Psychother
Psychosom.
2000;
69:329-334.
21.
Kirwan
M,
Armstrong
D.
Investigation
of
burnout
in
a
sample
of
British
general
practitioners.
Br
J
Gen
Pract.
1995;
45:
259-260.
22.
Linzer
M,
Visser
MRM,
Oort
FJ,
et
al.
Predicting
and
preventing
physician
burnout:
results
from
the
United
States
and
the
Neth-
erlands.
Am
J
Med.
2001;
111:
170-175.
|

