Elias A. Sarru' M.D, M.S, A.A.F.P, A.B.F.P.
Saudi Aramco Primary Care Division
Elias A. Sarru' M.D, M.S, A.A.F.P, A.B.F.P.
Saudi Aramco Primary Care Division,
31311
Abqaiq, P.O. Box: 864, Kingdom of Saudi
Arabia
Tel: 966-3-572-7286, Fax: 966-3-877-8787
E-mail: sarruea@hotmail.com;
sarruea@exchange.aramco.com.sa
|
|
ABSTRACT
Gynecomastia
is a strictly male condition and is
the most common cause of male breast
enlargement. Gynecomastia is predominantly
benign; however, remote possibilities
of underlying malignancy warrants
further investigation, especially
in the middle aged and elderly population.
True prevalence amongst the Saudi
population is not known, and in reporting
this case in a middle-aged Saudi man
we tried to observe any differences
in clinical manifestation from those
reported in literature, and highlight
the needed diagnostic work-up and
treatment in clinically indicated
cases.
|
Keywords: Gynecomastia,
Saudi population, clinical manifestation,
diagnostic work-up and therapeutic modalities.
Gynecomastia
results from proliferation of the glandular
breast compartment triggered by several
endogenous, and occasionally by exogenous,
factors [1]. Often, gynecomastia is the
result of absolute imbalance between estrogen
and androgen action at the breast tissue
level. Estrogens stimulate and androgens
inhibit breast glandular development [1,
2]. Most of the cases are benign whether
in infancy, pre-pubertal, pubertal and even
in adults. However, occasionally gynecomastia
might be due to the underlying pathologic
process of male breast cancer especially
in the elderly population with prolonged
exposure to female hormones, positive family
history, or patients with reduced testicular
function (Kleinfelter's Syndrome) [1, 2].
Age, family history, drug/medication history,
clinical manifestation and specific diagnostic
modalities remain crucial in differentiation
and treatment. Presenting a case of gynecomastia
among middle-aged Saudi men and reviewing
related literature, we aim towards increasing
the awareness of such a clinical entity
and highlight the work-up and treatment
when needed.
A 51 year old Saudi male
presented to our out-patient clinic with
mild pain and swelling of his right breast
of 6 weeks' duration. He voluntarily expressed
his reluctance to seek medical advice for
the past few weeks saying, "I thought
it would go away." Patient is a smoker
(30 packets a year). Family history, past
medical, surgical and drug history was unrevealing.
Examination revealed a 2.5 cm x 1.5 cm firm,
mildly tender sub-areolar mass with regular
borders and free from underlying and overlying
tissues, normal nipple and no lymph nodes
were felt. TSH, liver function test, renal
and chest X-ray were all normal. Mammography
report noted: "2.9 cm x 1.3 cm retro-areolar
right breast mass likely related to cancer."
A fine needle aspiration by a general surgeon
followed and the pathology report revealed
"Few clusters of ductal cells with
a few single epithelial cells." Afterwards,
an open right breast excision was done and
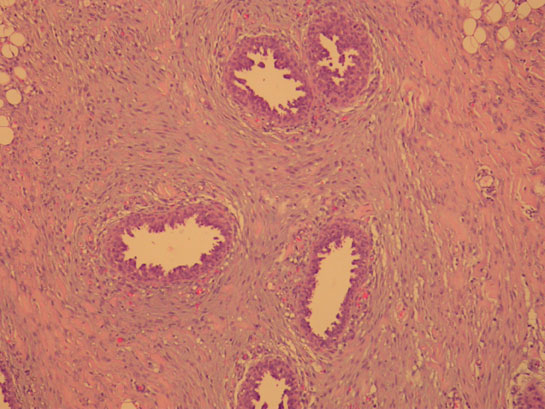
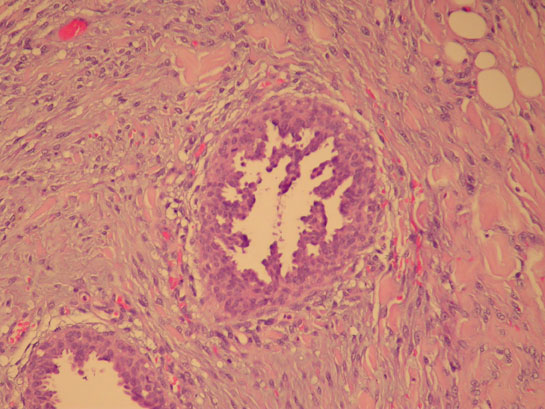
the pathology report noted the following:
"Several ductular structures lined
by hyperplastic ductal epithelium with papillary
projections and micro-papillary formations
embedded within connective tissue stroma
featuring an area of basophilic myxoid stroma
around ducts and intervening collagenous
fibrillary stroma. No features of malignancy
detected. The appearance is typical of gynecomastia."
Fig 1,2
|
|
Gynecomastia is predominantly
unilateral and quite prevalent among infants,
pubertal and to a lesser extent amongst
the elderly population. Female hormone estrogen
is the main factor in breast glandular proliferation
needed for breast enlargement in both sexes[1].
In males, estrogen is naturally counter-balanced
by male hormones androgens. Changing the
balance between the two sex hormones due
to several causes (Table 1),
enhanced sensitivity of breast tissue to
estrogen and insensitivity to androgens
lead to breast enlargement as well[1, 2].
Not all breast enlargements are due to hormonal
imbalance. Many overweight and obese teens
and adults have enlarged bilateral breasts
due to increase fat and not breast tissue.
This is called pseudo-gynecomastia and usually
disappears only when individuals involved
lose weight.
Neonatal and pubertal
cases of gynecomastia remain the most common
and usually resolve spontaneously in a couple
of weeks to two years, respectively. Reassurance,
patient and relative education of the physiologic
basis of the condition and periodic follow-up
is all that is needed.
However, gynecomastia
in pre-pubertal [3] and elderly age groups
[4, 5, 6] warrants further investigations
as clinically indicated. Long-term direct
or even indirect exposure to estrogen has
been associated with some gynecomastia cases
in pre-pubertal children. Testicular cancers,
primary gonadal failure (Kleinfelter's Syndrome),
secondary hypogonadism (mumps orchitis,
orcheoctomy cases) can lead to gynecomastia
due to decreased androgens. However, liver
cirrhosis, lung cancer, hyperthyroidism
and patients on dialysis have been associated
with increased levels of free estrogen as
a plausible cause of gynecomastia seen in
some of these patients. Finally, drug and
medication history should be reviewed as
another cause of gynecomastia in adults
[1, 7] (Table 1).
Male breast cancer, though
very rare, does exist. It accounts for 0.2%
of all cancers and 1% of all breast cancers
[4, 5, 6]. Our patient had a negative family
history and/or risk factors for male breast
cancer. Physical exam was also reassuring;
the mass felt concentric to the nipple without
nipple changes, well delineated borders
and not fixed to underlying tissues and
overlying skin. Initial work-up was negative,
and the mammography report was nonconclusive
towards either diagnoses. Fine needle aspiration
remains important in the diagnostic armamentarium
of breast lumps, yet literature points to
some false negative results [4]. Final diagnosis
came through the pathology report of the
excised breast tissue that ruled out malignancy
and detailed the typical appearance of gynecomastia.
The etiology behind our patient's gynecomastia
might be explained on the basis of either
increased estrogen sensitivity or decreased
sensitivity of breast tissue to endogenous
androgen.
Finally, open excision
of breast tissue has been widely used for
gynecomastia. Recently, new techniques in
the surgical approach utilizing the hyper-tumescent
power liposculpting have found to be successful
in treating gynecomastia and leaves little
scarring. Post-operative control of body
weight and exercise is needed for long-term
positive results and patient's self esteem
[8].
|
| 1. |
Braunstein,
G.D.: "Male Reproductive Endocrinology."
Cecil's Essentials of Medicine. Edited
by Thomas E. Andreoli, et al., W,B.
Saunders, 2001, pp. 575-582. |
| 2. |
Wilson,
J.D.: "Endocrine Disorders of the
Breast." Harrison's Principles
of Internal Medicine. Edited by Kurt
Isselbacker, et al., NewYork: McGraw-Hill,
1997, pp. 111-115. |
| 3. |
Felner,
E.I. and White, P.C.: Electronic Article
- Pre-pubertal Gynecomastia: Indirect
Exposure to Estrogen Cream. Pediatrics
Vol.105(4) e55;2000. |
| 4. |
Matias,
K.P.: An Unexpected Finding: Male Breast
Cancer is and Often Overlooked. OncoLog.49(4):2004.
|
| 5. |
Volpe,
C.M., et al.: Unilateral Male Breast
Masses: Cancer Risk and Their Evaluation
and Management. Am Surg; 65(3):250-253;
1999. |
| 6. |
Elias,
S.A., Faysal, M., Samir, A.S.: Male
Breast Cancer, Case Report and Brief
Review. Middle East Journal of Family
Medicine; 2(4), 2004. |
| 7. |
Tanner,
L.A. and Bosco, L.A.: Gynecomastia Associated
with Calcium Channel Blockers Therapy.
Arch.of Int.Med; 1988, 148(2): p. 379-80. |
| 8. |
Schafer,
J.B. and Shane, R.: Male Breast Liposuction
Today: Hypertumescent Power Liposculpting
- A 700 - Case Retrospective Study.
The American
Journal of Cosmetic Surgery; 22(4):
260-266, 2005 |
. |