|
|
 |
| ............................................................. |
|
|
| ........................................................ |
| From
the Editor |

|
Editorial
A. Abyad (Chief Editor) |
|
|
|
|
........................................................ |
Original
Contribution / Clinical Investigation
|
|
<-- Kuwait -->
Hyperglycemia
In Pregnancy in Arab Population, Kuwait Oil
Company Hospital, Kuwait
[pdf
version]
Hany M. Aiash, Sameh F. Ahmed,
Amro Abo Elezz
<-- Jordan -->
Ischiofemoral
impingement syndrome , incidence and clinical
importance
[pdf
version]
Jamil S. Shawaqfeh, Maysoon Banihani, Hend Harahsheh,
Ashraf Tamimi,
Abdulaziz Bawazir
<-- Abu Dhabi -->
Assessment
of behaviors, risk factors of Diabetic foot
ulcer and footwear safety among diabetic patients
in primary care setting, Abu Dhabi, UAE
[pdf version]
Osama Moheb Ibrahim Mohamed, Nwanneka E. O.
Ofiaeli, Adnan Syeed, Amira Elhassan,
Mona Al Tunaiji, Khuloud Al Hammadi, Maryam
Al Ali
<-- Nepal -->
Determinants
and Prevalence of Stunting Among Rural Kavreli
Pre-school Children
[pdf
version]
Kharel Sushil, Mainalee Mandira, Pandey Niraj
DOI:
<-- Qatar -->
Medical
and Psychological Associations with Nocturnal
Enuresis in Children in Qatar
[pdf version]
Ahmed Mohamed Kahlout, Hayam Ali AlSada
|
........................................................
International Health
Affairs
|
|
<-- Turkey -->
Aging
Syndrome
[pdf
version]
Mehmet Rami Helvaci, Orhan Ayyildiz, Orhan Ekrem
Muftuoglu, Mustafa Yaprak
Abdulrazak Abyad, Lesley Pocock
|
........................................................
|
Chief
Editor -
Abdulrazak
Abyad
MD, MPH, MBA, AGSF, AFCHSE
.........................................................
Editorial
Office -
Abyad Medical Center & Middle East Longevity
Institute
Azmi Street, Abdo Center,
PO BOX 618
Tripoli, Lebanon
Phone: (961) 6-443684
Fax: (961) 6-443685
Email:
aabyad@cyberia.net.lb
.........................................................
Publisher
-
Lesley
Pocock
medi+WORLD International
11 Colston Avenue,
Sherbrooke 3789
AUSTRALIA
Phone: +61 (3) 9005 9847
Fax: +61 (3) 9012 5857
Email:
lesleypocock@mediworld.com.au
.........................................................
Editorial
Enquiries -
abyad@cyberia.net.lb
.........................................................
Advertising
Enquiries -
lesleypocock@mediworld.com.au
.........................................................
While all
efforts have been made to ensure the accuracy
of the information in this journal, opinions
expressed are those of the authors and do not
necessarily reflect the views of The Publishers,
Editor or the Editorial Board. The publishers,
Editor and Editorial Board cannot be held responsible
for errors or any consequences arising from
the use of information contained in this journal;
or the views and opinions expressed. Publication
of any advertisements does not constitute any
endorsement by the Publishers and Editors of
the product advertised.
The contents
of this journal are copyright. Apart from any
fair dealing for purposes of private study,
research, criticism or review, as permitted
under the Australian Copyright Act, no part
of this program may be reproduced without the
permission of the publisher.
|
|
|
| April/May 2017
- Volume 15, Issue 3 |
|
|
Determinants and Prevalence
of Stunting Among Rural Kavreli Pre-school Children
Kharel Sushil
(1)
Mainalee Mandira (2)
Pandey Niraj (3)
(1) Lecturer, Department of Physiology,
Kathmandu Medical College and Teaching Hospital,
Kathmandu, Nepal
(2) Community Social Worker, Kavre
(3) Department of Anatomy, KMCTH
Correspondence:
Sushil
Kharel
Lecturer, Department of Physiology,
Kathmandu Medical College and Teaching Hospital,
Kathmandu,
Nepal
Email: drsushilkharel@gmail.com
|
Abstract
Background: Stunting is a reduced
growth rate in human development. It is
"height for age" value to be
less than two standard deviations of the
WHO Child Growth Standards median. Different
studies have shown that inadequate nutrient
intake, infections, unsafe water and poor
child care are among its main determinants.
In rural Nepal, stunting in children is
one of the most serious public health
concerns.
Aims and Objective: The objective
of this study was to find the prevalence
of stunting including severe stunting
and its determinants in pre-school children
aged 3-4 years in Kharelthowk VDC, Nepal.
Materials and Methods: A community
based cross-sectional survey was conducted
from July 2016 to January 2017 with systematic
random sampling technique. Total 464 pre-school
children of rural Kharelthowk VDC( Kavre
district), both males and females of age
between 3-4 years were enrolled in the
study. A structured questionnaire was
used to obtain information on socioeconomic
characteristics and life style factors
of children. WHO Anthro Software V3.2.2
was used for analyzing anthropometric
parameters of the children and Statistical
package for Social Sciences (SPSS) Windows
version 21 was used to analyze the data.
Result: The prevalence of stunting
in pre-school children was 46.9%. The
prevalence of stunting was significantly
higher among male children (51%) than
female children (42.7%). The study revealed
that stunting was significantly associated
with inadequate nutrition intake, infections,
poor child care and socio-economic status
of the family. Conclusion: The magnitude
of stunting is very high compared to developed
countries. Thus, proper attention should
be given for the intervention on causes
of stunting among pre-school children
in order to avoid further risks in future.
Key words: Stunting; Pre-school
children; Kavre
|
Stunting in pre-school children is associated
with adverse physiological consequences, including
poor cognition and educational achievements,
lost productivity and, when accompanied by huge
weight gain later in childhood(1). In developing
countries, it is estimated that 29% of children
aged less than five years (under-five children)
are stunted [<-2 standard deviation (SD)
height-for-age] or malnourished. Although stunting
has declined recently, prevalence is still extremely
high, especially in South Central Asia, which
alone accounts for about half of the global
problem(2). Child malnutrition is affected by
several determinants, such as intrauterine growth
retardation, lack of exclusive breastfeeding,
inappropriate complementary feeding, and continuous
attacks of infectious illnesses, food unavailability,
and micronutrient deficiencies(3). Although
the pathogenesis of stunting is not yet well-understood,
many studies have shown that inadequate nutrient
intake, infections, unsafe water and poor child
care, literacy rate of mothers, are among its
main determinants(4). Other factors in developing
countries include low socioeconomic status,
residence and poor access to health care services(5,
6). There is a wide variation in rates of malnutrition
throughout Nepal, both ecologically and regionally.
Nepal Demographic and Health Survey indicates
that more rural children are stunted (low height
for age), 42% than urban children (27%). Regional
variation in nutritional status of children
is substantial. Stunting levels are very high
in the mountains (53 %) (7).
The present analyses describe levels and trends
of stunting in pre-school children based on
the WHO standards. Moreover, while the earlier
research covered only stunting in urban areas
and reported the trends, the present study was
focused on the rural scenario of childhood stunting.
A
cross-sectional
community-based
study
was
conducted
in
pre-school
children
of
Kharelthowk
VDC.
The
study
was
carried
out
from
July
2016
to
January
2017.
Five
trained
volunteers
were
actively
involved
in
collecting
the
data
of
pre-school
children.
Informed
written
consent
was
taken
from
the
parents/guardian
and
school
authority
and
Helsinki
guidelines
were
followed.
A
self-designed
structured
questionnaire
regarding
lifestyle
factors
of
child,
economic
status
of
family,
etc
was
given
to
them.
Anthropometric
assessment
was
done,
their
weight,
height,
head
circumference,
mid-upper
arm
circumference
were
measured
three
consecutive
times.
Later
on,
mean
was
taken
as
their
actual
weight
and
height,
which
helped
in
calculating
the
BMI
(body
mass
index).
Anthropometric
measurement
was
done
by
LG
digital
weighing
machine
(with
a
difference
of
only
20
grams),
by
Stadiometer
and
non
stretchable
measuring
tape.
The
condition
of
the
weighing
machine
was
checked
then
was
kept
on
firm
flooring
(heavy
clothing
and
shoes
were
removed).
Children
were
told
to
stand
with
both
feet
in
the
center
of
the
scale
and
weight
was
recorded.
Height
measurement
was
done
by
Stadiometer;
children
were
asked
to
stand
up
straight
with
feet
and
heels
together
keeping
the
heels
back
against
the
upright
section
of
the
stadiometer
(arms
relaxed
by
sides).
Children
were
asked
to
look
straight
ahead
at
the
marker.
Three
standard
indices
of
physical
growth
given
by
WHO-Height-for-age
(Stunting),
Weight-for-age
(Underweight)
and
weight-for-height
(Wasting)
that
described
the
nutritional
status
of
children
was
considered
in
this
study.
WHO
Classification
(8).
Stunting:
Height
for
age
<
-2
Standard
Deviations
(SD)
of
the
WHO
growth
standard
Median
Underweight:
Weight
for
age
<
-2
Standard
Deviations
(SD)
of
the
WHO
growth
standard
Median
Wasting:
Weight
for
Height
<
-2
Standard
Deviations
(SD)
of
the
WHO
growth
standard
Median
Overweight:
Weight
for
Height
>
+
2
Standard
Deviations
(SD)
of
the
WHO
growth
standard
Median
Inclusion
criteria:
The
pre-school
children
aged
between
3
to
4
years.
Exclusion
criteria:
The
children
who
were
not
in
good
health
and
uncooperative.
Analysis
was
done
by
universally
accepted
WHO
Anthro
Software
Version
3.2.2
and
SPSS
Version
21.
Z
test
was
used
to
calculate
the
P
value.
P-value
of
<
0.05
was
considered
as
statistically
significant
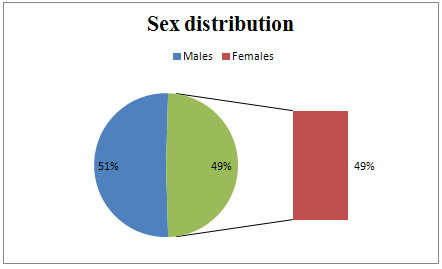
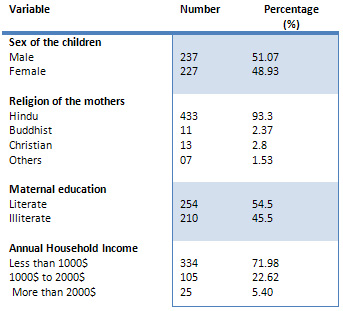
A
total
of
464
pre-school
children
aged
between
3-4
years
were
enrolled
in
the
study.
Of
these
464
participants
237(51.07%)
were
males
and
227(49.93%)
were
females
(Figure
1).
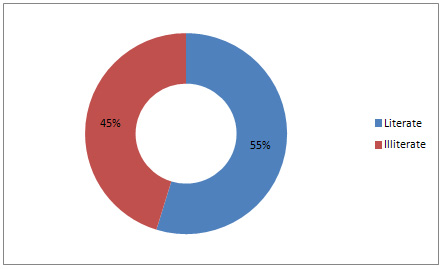
Among
the
mothers
of
participants,
54.5%
(254)
were
literate
and
45.5%
(210)
were
illiterate
(Figure
2).
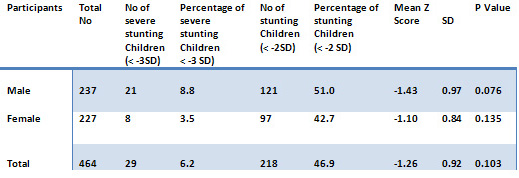
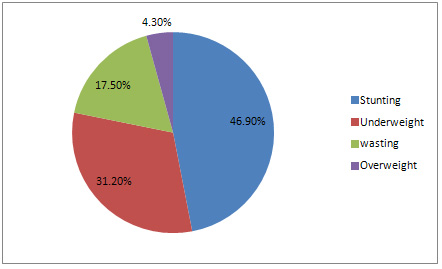
Prevalence
of
overall
stunting
was
46.9%
(218).
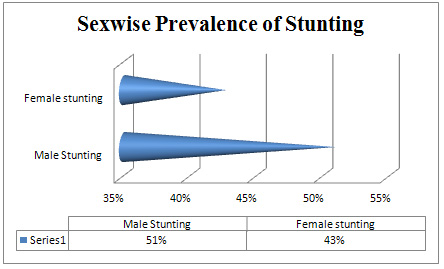
Prevalence
of
severe
stunting
in
males
and
females
were
8.8%
and
3.5%
respectively.
Males
were
more
stunted
as
compared
to
females.
The
prevalence
of
stunting
in
male
and
female
population
compared
to
its
own
counterpart
was
51%
and
42.7%
respectively
(Table
1).
The
prevalence
of
underweight
and
wasting
of
the
study
population
was
31.2%
and
17.5%
respectively
whereas
overweight
was
among
4.3
%
of
the
study
population
(Figure
4).
Figure
1:
Sex
wise
distribution
of
the
pre-school
children
Figure
2:
Literacy
rate
among
mothers
of
pre-school
children
in
the
study
population
Table
1:
Weight-for-height
Stunting
in
the
study
population
(95%
CI)
Figure
3:
Comparison
of
Stunting
among
male
and
female
pre-school
children
in
the
study
population
Figure
4:
Prevalence
of
stunting,
underweight,
overweight
and
wasting
among
study
children
(3-4
Years
of
age)
Table
2:
Socio-demographic
characteristics
of
study
children
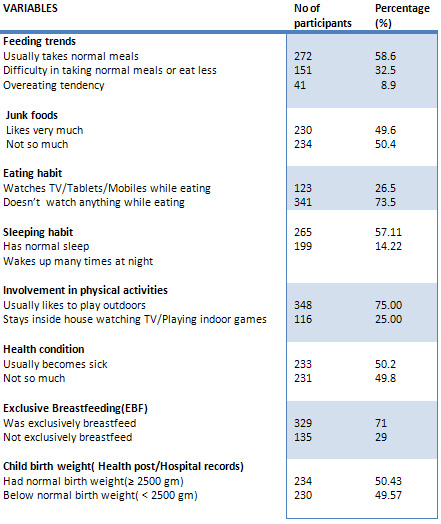
Table
3:
Life
style
factors
and
health
condition
of
the
children
In
developing
countries
like
Nepal,
stunting
in
children
has
become
a
public
health
concern
in
recent
times
due
to
its
bad
impact
on
the
health
of
the
child
in
the
future.
People
are
still
unaware
of
the
situation
and
this
may
lead
to
epidemic
causing
increase
risk
of
diabetes,
hypertension
and
other
diseases
in
future.
In
the
present
study
the
average
age
of
the
child
was
3.5±
0.2
years.
The
youngest
child
was
36
months
whereas
the
oldest
among
study
population
was
48
months.
A
study
in
Andhra
Pradesh,
India
assessed
1013
tribal
children
and
found
that
48.27%
were
stunted
(9).
This
study
showed
similar
results
to
our
study
which
showed
46.9%
of
children
of
age
3-4
years
were
stunted.
Bisai
et
al.
found
the
overall
prevalence
of
stunting
was
47.8
%
in
3-6
years
children(10).
Another
study
from
Rajasthan
reported
that
60
%
were
stunted
among
rural
children
less
than
3
years
(11).
Rao
et
al.
found
that
51.6%
were
stunted
among
tribal
pre-school
children(12).
In
a
study
in
Saudi
Arabia
it
showed
that
a
prevalence
of
stunting
was
10.9%
in
under
5
children
which
is
far
lower
as
compared
to
us
and
our
region(13).
One
noticeable
aspect
of
our
study
is
significantly
higher
prevalence
of
stunting
among
boys
as
compared
with
girls.
Rao
et
al.
in
their
study
also
had
found
a
higher
prevalence
of
stunting
(54.4%
vs.
48.8
%)
among
boys(12).
But
Stalin
et
al.
in
his
study
found
that
malnutrition
was
more
prevalent
among
girls
than
boys
in
Tamilnadu,
India
(62.6%
vs.
44%)
(14).
The
study
clearly
showed
that
the
stunting
was
significantly
associated
with
feeding
habit,
sleeping
condition,
health
condition
of
child,
child
birth
weight
(Table
3)
and
lower
socio-economic
status
of
the
family
(Table
3).
The
prevalence
of
stunting
found
in
this
study
is
very
high
as
compared
to
developed
countries.
This
is
due
to
poor
child
nutrition,
illness,
low
birth
weight
of
child
and
poor
economic
conditions.
Thus,
proper
attention
should
be
given
for
the
intervention
on
causes
of
stunting
among
pre-school
children
in
order
to
avoid
the
diseases
in
future.
The
trend
of
studies
in
developing
countries
is
only
focused
in
urban
areas.
The
problem
of
stunting
in
children
is
more
in
rural
areas
so
this
type
of
study
should
be
concentrated
more
in
rural
areas.
Acknowledgements
I
express
my
deep
sense
of
gratitude
to
my
participants
who
were
very
little
children
without
their
cooperation
this
study
might
not
have
been
successful.
A
special
thanks
to
Mr.
Sunil
Kharel
(Head
of
the
Department
of
Economics,
Uniglobe
College)
for
his
help
and
support
in
statistical
analysis.
1.
Victora
CG,
Adair
L,
Fall
C
et
al.,
for
the
Maternal
and
Child
Undernutrition
Study
Group
(2008)
Maternal
and
child
undernutrition:
consequences
for
adult
health
and
human
capital.
Lancet
371,
340-57.
2.
United
Nations.
4th
report-the
world
nutrition
situation:
nutrition
throughout
life
cycle.
Final
report
to
the
ACC/SCN
by
the
Commission
on
the
Nutrition
Challenges
of
the
21st
Century.
New
York,
NY:
United
Nations,
2000:1-144.
(http://www.unscn.org/layout/
modules/resources/files/rwns4.pdf,
accessed
on
10
November
2010).
3.
Ahmed
T,
Ahmed
AMS.
Reducing
the
burden
of
malnutrition
in
Bangladesh.
BMJ
2009;
339:
b
4490.
4.
Stewart
CP,
Iannotti
L,
Dewey
KG,
et
al.
Contextualising
complementary
feeding
in
a
broader
framework
for
stunting
prevention
[Internet].
Matern
Child
Nutr
2013;9(Suppl.
2):27-45.
http://www.ncbi.nlm.nih.gov/
pubmed/24074316
(10
December
2014,
date
last
accessed)
5.
Abubakar
A,
Uriyo
J,
Msuya
SE,
et
al.
Prevalence
and
risk
factors
for
poor
nutritional
status
among
children
in
the
Kilimanjaro
region
of
Tanzania
[Internet].
Int
J
Environ
Res
Public
Health
2012;9:3506-18.
Multidisciplinary
Digital
Publishing
Institute.
http://www.mdpi.com/1660-
4601/9/10/3506/htm
(18
July
2014,
date
last
accessed)
6.
Masanja
H,
Schellenberg
JA,
de
Savigny
D,
et
al.
Impact
of
Integrated
Management
of
Childhood
Illness
on
inequalities
in
child
health
in
rural
Tanzania
[Internet].
Health
Policy
Plan
2005;20(Suppl.
1):i77-84.
http://www.ncbi.
nlm.nih.gov/pubmed/16306073
(27
July
2014,
date
last
accessed)
7.
Population
Division,
Ministry
of
Health
and
Population,
Department
of
Health
Services,
Government
of
Nepal.
Nepal
Demographic
and
Health
Survey
(NDHS),
report.
[Internet].
2011.
Available
from:
h
t
t
p
:
/
/
w
w
w.
m
o
h
p
.
g
o
v.
n
p
/
e
n
g
l
i
s
h
/
p
u
b
l
i
c
a
t
i
o
n
/
NDHS%202011%20Full%20version.pdf
8.
World
Health
Organization.
WHO
child
growth
standards:
length/height-for-age,
weight-for-age,
weight-for-height
and
body
mass
index-for-age:
Methods
and
development.
Geneva,
Switzerland:
World
Health
Organization;
2006.
Available
at
http://www.who.int/childgrowth/publications/technical_report_pub/en/index.html
9.
Sukhdas
G,
Challa
S,
Bhatia
P,
Rao
AR,
Rao
PK.
Nutritional
status
of
tribal
children
in
Andhra
Pradesh.
Int
J
Med
Res
Health
Sci
2014;
3(1):
76-9.
10.
Bisai
S,
Bose
K,
Dikshit
S.
Under-nutrition
among
slum
children
aged
3-6
years
in
Midnapore
town,
India.
Internet
J
Biol
Anthropol
2008;
2
(2).
Available
at:
https://ispub.com/IJBA/2/2/10564.
11.
Bisla
G,
Archana
Kapoor
M.
Nutritional
status
of
Toddlers
(1-3
Years)
of
Rural
area
of
Niwai
Tehsil,
Tonk,
Rajasthan,
India.
Int
J
Trop
Med,
2012;
7
(5,6):
157-64.
12.
Rao
VG,
Yadav
R,
Dolla
CK,
Kumar
S,
Bhondeley
MK
&
Ukey
M.
Undernutrition
&
childhood
morbidities
among
tribal
preschool
children.
Indian
J
Med
Res
2005;
122(1):
43-7.
13.
Mohammad
et
al.
Prevalence
of
malnutrition
in
Saudi
children:
a
community-based
study.
Ann
Saudi
Med.
2010
Sep-Oct;
30(5):
381-385.doi:
10.4103/0256-4947.67076
14.
Stalin
P,
Bazroy
J,
Dimri
D,
Singh
Z,
Senthilvel
V,
Sathyanarayanan
S.
Prevalence
of
Underweight
and
its
Risk
Factors
among
Under
Five
Children
in
a
Rural
Area
of
Kancheepuram
District
in
Tamil
Nadu,
India.
IOSR-J
Dental
and
Med
Sci
2013;
3
(6):
71-4.
|
|
.................................................................................................................

|
| |
|
