|
Presenting a case of male breast cancer
among male Saudi population and reviewing related literature,
we aim to highlight the importance of increased awareness towards
the existence of such disease among the Saudi population, and
to observe any differences in clinical manifestation from those
reported in literature.
Case Report
A seventy eight year old Saudi male presented to our outpatient
clinic with left breast pain of two month's duration. Examination
revealed a 2 x 1 cm hard medial sub-areola tender mass with
irregular borders almost fixed to underlying structure. This
was associated with mild left nipple retraction and a 1 x 1
cm non-tender left axillary node. The
mammography report noted: 'A 1.5 cm stellate mass of left breast
consistent with carcinoma. Two small lymph nodes present at
left upper outer quadrant, one dense in craniocaudal view and
may be involved with metastasis.' Carcino-embryonic antigen
(CEA), liver function tests, calcium, prostatic specific antigen,
right upper quadrant ultrasound and chest x-ray were reported
as normal. A fine needle aspiration revealed findings consistent
with invasive carcinoma. The patient underwent modified left
radical mastectomy with right axillary sampling.
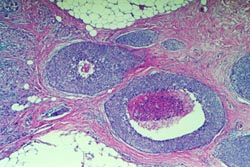
Histopathological examination of the tumor revealed infiltrating
ductal carcinoma, moderately differentiated (Grade 2 according
to Modified Scarff- Bloom-Richardson grading system). There
were cords and nests of malignant epithelial cells embedded
within dense collagenous stroma; some are surrounding normal
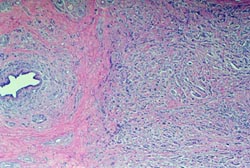
non-neoplastic ducts (Figure 1). In addition, there were foci
of intraductal comedo carcinoma featuring dilated ducts lined
by malignant epithelial cells with central necrosis (Figure
2).
|